Download
1 / 13
130 likes | 748 Views
Renin-Angiotensin System (RAS) Drugs. Key Slides. Why do we use RAS drugs?. ACE inhibitors and A2RAs are variously licensed for: Hypertension Heart failure Treatment post-MI Diabetic nephropathy Prevention of CV events in those at high risk

E N D
Renin-Angiotensin System (RAS) Drugs Key Slides
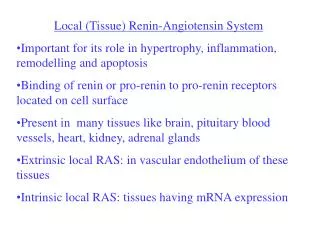
Why do we use RAS drugs? ACE inhibitors and A2RAs are variously licensed for: Hypertension Heart failure Treatment post-MI Diabetic nephropathy Prevention of CV events in those at high risk The exact indications covered and wording used for each drug are very variable They are used in various conditions: Hypertension Heart failure / left ventricular dysfunction Treatment post-MI Diabetes Chronic kidney disease (CKD) • Prescribing can be: • ACE inhibitor alone • A2RA alone • ACE inhibitor + A2RA
Why is RAS drug choice important?QUALITY and VALUE (1) Decisions are guided by four factors: • Efficacy • Safety • Patient factors • Cost QUALITY What is evidence-based practice for use of RAS drugs? • Evidence-based position is that ACE inhibitors are first-line choices • A2RAs are an alternative to ACE inhibitors if RAS drugs are indicated but an intractable cough requires discontinuation of the ACE inhibitor. EFFICACY SAFETY COST PATIENT FACTORS
Why is RAS drug choice important?QUALITY and VALUE (2) • VALUE • “The NHS must demonstrate that it is making the most effective use it can of public money to deliver quality healthcare.” • NHS Institute for Innovation and Improvement, http://www.productivity.nhs.uk/ • Generic ACE inhibitors are less expensive than A2RAs • Patent expiry for A2RAs are as follows www.ukmi.nhs.uk • - Losartan March 2010 • - Valsartan May 2011 • - Eprosartan April 2012 • - Candesartan April 2012 • - Irbesartan October 2013 • - Telmisartan January 2017 • - Olmesartan February 2017
NICE guidance: ACE inhibitors first-lineNICE CG34 Hypertension, 2006; NICE CG5 Heart Failure, 2003; NICE CG48 MI: secondary prevention, 2007; NICE CG87 Type 2 diabetes, 2009; NICE CG73 Chronic kidney disease, 2008 • NICE guidance advocates RAS drugs in: • Hypertension • Heart failure • Treatment post-MI • Type 2 diabetes • Chronic kidney disease (CKD) • Current NHS policy (NICE guidance) for each of these indications place ACE inhibitors first-line where RAS drugs are indicated • They reserve A2RAs for patients in whom RAS drugs are indicated but ACE inhibitors have to be discontinued because of an intractable cough.
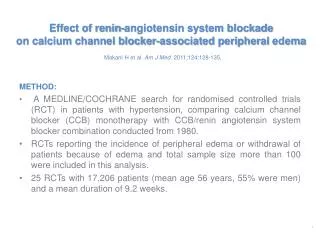
ONTARGET (1)N Engl J Med 2008;358:1547–59, http://www.npci.org.uk/blog/?p=98 • Telmisartan 80mg od vs. ramipril 10mg od vs. both in patients with vascular disease or diabetes with end organ damage (but no heart failure) • n=25,620; median follow-up 56 months • 85% had CVD, 69% hypertension, 38% diabetes • No significant difference in primary outcome (CV death, MI, stroke or hospitalisation for HF) between telmisartan, ramipril or both • telmisartan non-inferior to ramipril; combination no better than monotherapy • Compared with telmisartan more ramipril patients discontinued due to: • cough; 4.2% vs. 1.1%, absolute difference 3.1%, NNH 32 • angioedema; 0.3% vs. 0.1%; absolute difference 0.2%, NNH 500 • Compared with ramipril more telmisartan patients discontinued due to: • hypotensive symptoms; 2.7% vs. 1.7%; absolute difference 1%, NNH 100
A2RA instead of ACE inhibitor:discontinuation due to cough in ONTARGETN Engl J Med 2008;358:1547–59 These 96 people will not stop treatment due to a cough within 4.5 years whether they take an ACE inhibitor or an A2RA. These 3 people will be ‘saved’ from stopping treatment due to a cough within 4.5 years because they take an A2RA instead of an ACE inhibitor. This 1 person will stop treatment due to a cough within 4.5 years whether they take an ACE inhibitor or an A2RA. The images have been produced using Dr Chris Cates’s software VisualRx 3.0. More information can be obtained from the website www.nntonline.net
ONTARGET (2)N Engl J Med 2008;358:1547–59, http://www.npci.org.uk/blog/?p=98Mann JFE, et al. Lancet 2008;372:547–53 • Combination was no more effective than treatment with ramipril or telmisartan alone and was associated with more discontinuations due to hypotension, syncope, diarrhoea and renal impairment • Primary renal outcome (composite of dialysis, doubling of serum creatinine and death) increased with combination • HR 1.09; 95% CI 1.01 to 1.18, P=0.037; NNH 91 (vs. ramipril) • Secondary renal outcome (dialysis or doubling of serum creatinine) increased with combination • HR 1.24; 95% CI 1.01 to 1.51, P=0.038; NNH 215 (vs. ramipril) • Acute dialysis increased with combination • HR 2.19; 95% CI 1.13 to 4.22, P=0.020; NNH 562 (vs. ramipril) • Most ONTARGET patients did not have micro or macroalbuminuria, but in the subgroup that did there was no benefit of combination therapy.
Tolerability: the bottom-line • Cough is not as common with ACE inhibitors as we think: • Notable in HF often due to underlying condition; but NNH for discontinuation due to cough similar in hypertension and HF trials • Not all coughs require treatment discontinuation • Before switching from ACE to A2RA because of cough, are RAS drugs the only option? i.e. what about thiazides or CCBs for uncomplicated hypertension • About 30 people need to be treated with an A2RA rather than an ACE inhibitor for 56 months to prevent one person having to stop taking the ACE inhibitor because of cough • In other words a 3% absolute difference (from 4% to 1%) N Engl J Med 2008;358:1547–59 • So should >90% of RAS prescribing be for an ACE inhibitor? NICE full hypertension guideline 2006
Combination treatment: the bottom-line • Hypertension • Evidence suggests no benefit and worse outcomes in ONTARGET • Renal disease • Evidence suggests no benefit and worse outcomes in ONTARGET • NICE full guideline says no evidence to suggest increased effectiveness • If specialists are using in a minority of patients with proteinuria not responding to monotherapy, requires very careful monitoring • Heart failure • Evidence suggests reduced hospitalisations but no reduction in mortality and increased adverse effects • SIGN suggest possibly a specialist option in a minority of patients still symptomatic once ACE inhibitors and beta blockers are optimised • BUT real concerns about renal failure, which could be exacerbated by diuretic use in HF patients, requires very careful monitoring.
Overall summary • Need to focus on QUALITY and VALUE in RAS drug prescribing • Evidence-based position is that ACE inhibitors are first-line choice • ACE inhibitors have a more robust evidence base across all indications • No evidence that A2RAs are more effective in any indication • No evidence that A2RAs are safer in any indication • Generic ACE inhibitors are less expensive than A2RAs • A2RAs are an alternative to ACE inhibitors if RAS drugs are indicated but an intractable cough requires discontinuation of the ACE inhibitor • The tolerability of ACE inhibitors is better than we might think • NNH about 30 for discontinuation due to cough • Would it be unreasonable for >90% of RAS drug prescribing to be for ACE inhibitors? • Combination treatment has a very limited role • Should be undertaken by specialists only, with careful monitoring of renal function.