Download

1 / 26
260 likes | 596 Views
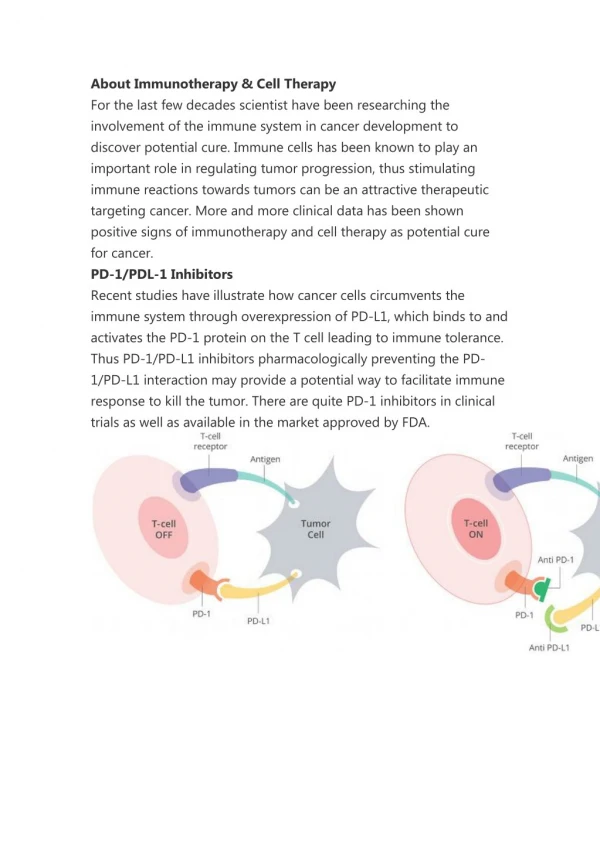
Allergy Symptom Response Following Conversion from Injection Immunotherapy to Sublingual Immunotherapy. CDR Timothy Clenney, MD, MPH Naval Medical Center Portsmouth Department of Otolaryngology/Head and Neck Surgery. Disclaimer.

E N D
Allergy Symptom Response Following Conversion from Injection Immunotherapy to Sublingual Immunotherapy CDR Timothy Clenney, MD, MPH Naval Medical Center Portsmouth Department of Otolaryngology/Head and Neck Surgery
Disclaimer The views expressed in this article are those of the author(s) and do not reflect the official policy or position of the Department of the Navy, Department of Defense, or the United States Government. .
Background Allergy immunotherapy has traditionally been administered via subcutaneous injection Interest in non-injection routes, such as the sublingual route have arisen out of concerns for safety and convenience. Non-injection routes may be of particular interest for active duty personnel due to logistical and safety considerations of immunotherapy administration outside the MTF. Passalacqua, G., C. Lombardi, and G.W. Canonica, Curr Opin Allergy Clin Immunol 2004; 4(1)
Background • Operational involvement in desert environments entails significant aeroallergen exposure • Allergy control impacts asthma as well as allergic rhinitis (AR) • During Initial Gulf war (1991), asthma was one of the most common causes of in-theater medical evacuation • Up to 78% of patients with asthma have AR and 38% of AR have asthma • Immunotherapy is often indicated when allergy and asthma cannot be controlled medically. Waibal KH. Allergic rhinitis in the Middel East. Military Medicine 2005 (170)
Background In Europe, sublingual immunotherapy (SLIT) has been regarded as a preferred alternative to subcutaneous immunotherapy since its introduction in 1986. In the United States, sublingual route is not FDA approved and is an “off-label” use. Although the efficacy and safety of SLIT are well established, no studies have examined symptom control in patients converted from injection immunotherapy to SLIT Leatherman BD, et al. Otolaryngol Head Neck Surg 2007;136
AIMS • Determine the allergy symptom response in patients converted from injection immunotherapy to SLIT • Assess allergy-related quality of life in a cohort of patients converted from injection immunotherapy to SLIT • Examine the effectiveness and utility of SLIT in a small group of active-duty military personnel
Methods Juniper EF, Thompson AK, Ferrie PJ, et al. Clinical and experimental allergy 2000; 30 (1) • Questionnaires were offered to a sample ENT allergy patients receiving SLIT that had previously been managed with injection immunotherapy • Four categories of allergy symptoms: • Eye Symptoms • Nasal Symptoms • Sleep Symptoms • Constitutional symptoms • Quality of life was assessed using a validated rhinoconjunctivitis QOL instrument
All patients continued current allergy medical treatments (antihistamines,etc) Multi-antigen SLIT was started on all patients using a standardized protocol⁴ Antigen treatment concentration was based upon the results of allergy in-vitro testing This study was approved by the Naval Medical Center Portsmouth institutional review board Methods
200 patients currently receiving SLIT 58 of the 200 had previously received injection immunotherapy 28 patients lost to follow-up or not available during the study period 30 patients receiving SLIT were invited to participate in this survey 100% agreed to participate Results
Results Nasal Symptoms • 30 (100%) reported nasal symptoms. • 22(73%) – Improved nasal symptoms • 8 (28%) – No change in nasal symptoms • 0 (0%) – Worsening of nasal symptoms P = 0.016
Results Eye Symptoms • 27 (90%) reported eye symptoms • 19 (70%) – Improved eye symptoms • 7 (26.9%) – No change in eye symptoms • 1 (3%) – Worsening of eye symptoms P < 0.001
Results Sleep Symptoms • 26 (86%) reported sleep symptoms • 12 (46%) – Improved sleep symptoms • 13 (50%) – No change in sleep symptoms • 1 (3%) – Worsening in sleep symptoms P=0.006
Results Constitutional Symptoms • 26 (86%) reported constitutional symptoms • 15 (58%) – Improved constitutional symptoms • 9 (35%) – No change in constitutional symptoms • 2 (7%) – Worsening of constitutional symptoms P = 0.008
Symptom Control Following Conversion to SLIT P = 0.016 P<0.001 P=0.008 P=0.006 Constitutional
SLIT in Active-Duty Military • 15 active-duty patients receiving SLIT • 8 previously on injection IT • 7 No previous immunotherapy • No reported adverse reactions • None discontinued therapy • 3 deployed while receiving SLIT
Concurrent Medical Therapy (military group)
Discussion • The primary objective of this study was to determine the self-reported clinical response to sublingual immunotherapy (SLIT) among patients previously managed with subcutaneous injected immunotherapy (SCIT). • The results of this study, though limited by small sample size, suggest that most patients can be converted from injection immunotherapy to sublingual immunotherapy with good symptom control.
Discussion • Specific symptom control reported by patients were consistent with rhinoconjuctivitis quality of life scores which suggested overall good quality of life based on a validated instrument. • These results are tempered by the fact that most patients continued to use allergy pharmocotherapy to manage symptoms. • Because military personnel are often unable to use injection immunotherapy due to logistical limitations, we evaluated the use SLIT in this group.
Discussion • In this smaller, separate analysis, military personnel using SLIT reported very good rhinoconjunctivitis quality of life scores, whether or not they previously received immunotherapy. • Concurrent pharmacotherapy was used less often by military personnel • The potential benefit here may be limiting medication side-effects
Conclusions Allergy patients receiving injection immunotherapy can be converted to SLIT with either improvement or no reduction in rhinoconjunctivitis symptom control. Patients converted from injection immunotherapy to SLIT report good overall quality of life Because it can be safely self-administered and efficacious, SLIT may be an ideal approach to allergy management when immunotherapy is indicated for military personnel.
References • Passalacqua, G., C. Lombardi, and G.W. Canonica, Sublingual immunotherapy: an update. CurrOpin Allergy ClinImmunol 2004; 4(1) • Leatherman BD, Owen S, Parker M, et al. Sublingual immunotherapy: Past, present, paradigm for the future? A review of the literature. Otolaryngol Head Neck Surg 2007;136 • Juniper EF, Thompson AK, Ferrie PJ, et al. Development and validation of the Mini Rhinoconjunctivitis Quality of Life Questionnaire. Clinical and experimental allergy 2000; 30 (1) • La Crosse Method, sublingual immunotherapy practice protocol, 2008. Allergychoices, inc La Crosse Wi.