Download
1 / 53
630 likes | 1.08k Views
RENAL REPLACEMENT THERAPY IN END-STAGE RENAL DISEASE. C K IJOMA. Outline. Definitions Classification Clinical features Treatment modalities: 1) Dialysis 2) Kidney Transplantation. NKF-K/DOQI* Definition of CKD KDIGO** Modifications (Amsterdam 2004.

E N D
RENAL REPLACEMENT THERAPY IN END-STAGE RENAL DISEASE C K IJOMA Lecture Med Students
Outline • Definitions • Classification • Clinical features • Treatment modalities: 1) Dialysis 2) Kidney Transplantation Lecture Med Students
NKF-K/DOQI* Definition of CKDKDIGO** Modifications (Amsterdam 2004 Chronic kidney disease defined as • kidney damagefor ≥ 3 months, as defined by structural or functional abnormalities of the kidney, with or without decreased GFR, manifest by either: • pathological abnormalities; or • markers of kidney damage, including abnormalities in the composition of the blood or urine, or abnormalities in imaging tests. • Kidney transplantation • GFR <60mL/min/1.73m2 for ≥ 3 months, with or without kidney damage. *National Kidney Foundation Kidney Disease Outcomes Quality Initiative **K/DIGO: kidney disease, increasing global outcome Lecture Med Students
NKF-K/DOQI* classification of CKD 2002 *National Kidney Foundation Kidney Disease Outcomes Quality Initiative Lecture Med Students
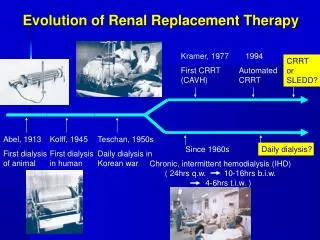
End Stage Renal Disease A clinical state in which there has been • An irreversible loss of endogenous renal function • Of a degree sufficient to render the patient permanently dependent upon renal replacement therapy (dialysis or transplantation) in order to avoid life threatening uraemia. Lecture Med Students
Uraemia Clinical and laboratory syndrome, reflecting dysfunction of all organ systems as a result of untreated and undertreated acute or chronic renal failure. Lecture Med Students
Renal replacement therapy • Dialysis a) haemodialysis b) peritoneal dialysis i) continuous ambulatory peritoneal dialysis (CAPD) ii) continuous cyclic peritoneal dialysis (CCPD) 2. Kidney transplantation Lecture Med Students
Treatment modalities for ESRD Lecture Med Students
Dialysis. Definition. Process of separating elements in solution by diffusion across a semipermeable membrane down a concentration gradient Principal process of removing end products of nitrogen metabolism (urea, creatinine, uric acid), and for repletion of bicarbonate deficit of metabolic acidosis associated with renal failure. Lecture Med Students
Indications to start dialysis • GFR ≤ 10 ml/min/1.73m2. (15 ml/min/1.73m2 in DM) • Pt loses stamina to sustain normal daily work and activity • Symptoms: nausea, vomiting, anorexia, fatiguability, diminished sensorium • Signs: pericardial friction rub, refractory pulmonary oedema, metabolic acidosis, foot or wrist drop, asterixis. Lecture Med Students
Preparation for haemodialysis • Vascular access temporary permanent Lecture Med Students
Haemodialysis • The extracorporeal circuit • The dialyzer • Water treatment • The dialysis machine • Dialysis prescription • Adequacy of HD: urea kinetic model, urea reduction ratio. Targets, UKM=1.3. URR≥70% Lecture Med Students
Haemodialysis circuit Lecture Med Students
Complications of haemodialysis • Anaphylactic and anaphylactoid reactions: First-use reactions, Re-use reactions, Bradykinin-mediated reactions (pts on ACEI dialyzed with AN69 dialyzers) • Microbial contamination • Hypotension • Hypertension • Cardiac arrhythmias Lecture Med Students
Complications of haemodialysis 2 • Sudden death (Vent fibrillation) • Muscle cramps • Restless leg syndrome • Dialysis disequilibruim syndrome • Seizures • Headache • Intradialytic haemolysis • Haemorrhage • Air embolism Lecture Med Students
Complications of haemodialysis 3 • Dialysis dementia • Dialysis arthropathy • Cystic degeneration of native kidneys Lecture Med Students
Peritoneal dialysis A technique whereby infusion of dialysis solution into peritoneal cavity is followed by variable dwell time and subsequent drainage Types of chronic PD • Continuous ambulatory peritoneal dialysis (CAPD) • Continuous cyclic peritoneal dialysis (CCPD) Lecture Med Students
Physiological Forces in PD Treatment Blood PD-Solution DiffusionFree solute movement with concentration gradient. ConvectionSolute transport driven by aquous fluid flow. OsmosisWater flows across a semi- permeable membrane driven by the concentration gradient of the 'indiffusible'osmotically active solutes. Solution Volume 25-40 mL/ kg Buffers HC03, lactate Electrolytes Na, Cl, Mg, Ca, K Osmotic Agent Glucose Peritoneum Lecture Med Students 16
Indications for chronic PD • ESRD • Choice • Poor vascular access for HD • Haematological disorders precluding use of heparin • Poor cardiovsacular status Lecture Med Students
Contraindications to chronic PD • Recent abdominal surgery • Extensive fibrosis of the peritonium • Abdominal aortic graft placement • Large individual Lecture Med Students
Complications of peritoneal dialysis • Peritonitis • Catheter tunnel infection • Damage to/perforation of abdominal viscera • Loss of protein in effluent Lecture Med Students
Kidney transplantation • Kidney transplantation is option in ESRD • Improves quality of life • Frees from chronic dialysis and restrictive diet • Long term mortality risk for transplant recipient 68% lower than for patients on dialysis • Projected increased life span of 3 to 17 years • Annual death rate 6.3 per 100 patient years for dialysis patients and 3.8 per 100 patient years for transplant patient Lecture Med Students
Sources of kidney. • Deceased donor (cadaver). • Living voluntary donor a) related (immediate and extended family) parent, sibling, son, daughter, aunt, uncle, cousin b) unrelated (longstanding relationship with patient) spouses, adopted/step family member, friend Lecture Med Students
Kidney donor evaluation General principles • Donation is safe for both donor and recipient • Primary focus is protection of wellbeing of prospective donor • Ensure donor has no disease that can be transmitted with the kidney • Donation based upon altruistic ideals and not driven by economic incentive Lecture Med Students
Preliminary workup • General medical screen for obvious contraindications hypertension diabetes mellitus Lecture Med Students
Tissue typing studies • Blood groups ABO and crossmatch (to check for preformed antibodies) • HLA crossmatch (recipient serum with donor T lymphocyte). Positive crossmatch predictive of acute rejection event resulting in hyperacute rejection • Tissue typing: (to determine degree of HLA matching between donor and recipient) Lecture Med Students
Laboratory tests • Complete blood count • Chemistry screen: E + U + creatinine, Plasma glucose, LFTs, lipid profile • Urinalysis and urine culture • Coagulation studies • 24 hour urine collection for creatinine clearance, proteinuria Lecture Med Students
Serology: HIV, CMV, EBV, HBV, HCV, • CXR, PPD , PAP, mamogram • ECG: Stress ECG and full cardiac assessment if patient is over forty years or history of heart disease in family • Lung function tests if smoker Lecture Med Students
Arterial imaging 2 kidneys of normal size and appearance Outline renal vascular and urinary drainage anatomy • Contrast angiography • Spiral CT • MR angiography Lecture Med Students
Screening for inherited renal disease • Family history of renal disease • ADPKD. >30 yr high resolution CT. 21-30 ?genetic • DM • Essential hypertension • ?kidney stone • Sickle cell trait Lecture Med Students
Psychological assessment • Donor’s motivation: voluntary • Good understanding of potential outcomes for both donor and recipient • Psychosocial history • Relationship between donor and recipient • Pressure and coercion • Presence of psychiatric disorder Lecture Med Students
Contraindication for live kidney donation • ?ABO incompatibility • ?HLA mis-match • Impaired kidney function • Significant non-orthostatic proteinuria (>200mg/24 hr) • Active malignancy • Active substance abuse • Severe chronic illness • pregnancy Lecture Med Students
Recipient evaluation • Candidate should have >5 yr life expectancy • Risk benefit evaluation • Diagnosis of correctable disease: coronary artery disease, infections- HIV, HBV, HCV, Tb, neoplasm • Strict protocol for transplantation in HIV and hepatitis Lecture Med Students
Blood tests • FBC + Diff + ESR • Blood group • Clotting profile • Chemistry: E + U + creatinine, LFT's, glucose • Lipid profile • Parathyroid hormone • Calcium • Tissue typing + crossmatch Lecture Med Students
Serology: CMV, EBV, HIV, HBV, HCV Cancer screen • Chest radiograph • Mammogram • PAP test • Stool occult blood • Digital rectal exam • sigmoidoscopy Lecture Med Students
Screen for infections • Life threatening infection • HIV • TB or positive PPD without adequate therapy • CMV Lecture Med Students
Gastrointestinal • HBsAg • HCV ab • Gastroduodenoscopy: PUD • pancreatitis • Cholecystitis Lecture Med Students
Cardiovascular • ECG • Cardiac assessment if over 40 • Angiogram to be performed on diabetic patients • IHD • CVD Lecture Med Students
Urological • VCUG: To see if there is any reflux and to ensure that the bladder is emptying completely • Ultrasonography • Cystoscopy • Retrograde urethrogram Lecture Med Students
Medical risk to recipient • BMI > 35 • ?age > 65 yr • HTN unresponsive to med management • DM Lecture Med Students
Associated recurrent disease in recipient • ADPKD and alports syndrome do not usually recur • FSGS, HUS, HSP, hereditary oxalosis recur soon • MPGN, scleroderma, IgA nephropathy, DM recur after several years Lecture Med Students
Psychological evaluation • Cognitive impairment • Recent alcohol or drug abuse • Psychiatric illness • Medication non-compliance Lecture Med Students
Contraindications to transplantation • Active malignancy • Terminal illness • Psychiatric illness • Recent MI • Drug and alcohol abuse • Active infection Lecture Med Students