Download
1 / 22

E N D
1. An idiots� guide Renal Replacement Therapy in Critical Care
2. �There�s nothing more dangerous than a resourceful idiot�
Scot Adams, American Cartoonist
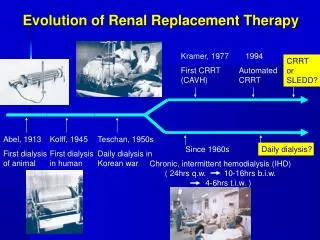
3. Removing badness from the blood First used in the Korean War
Dialysis, cf Greek �to pass through�
4. Indications
Oliguria (urine output <200 mL/12 h)
Anuria/extreme oliguria (urine output <50 mL/12 h)
Hyperkalaemia ([K] >6.5 mEq/L)
Severe acidaemia (pH <7.1)
Azotemia ([urea] >30 mg/dL)
Pulmonary oedema
Uraemic encephalopathy
Uraemic pericarditis
Uraemic neuropathy/myopathy
Severe dysnatraemia ([Na] <115 or >160 mEq/L)
Hyperthermia
Drug overdose with dialyzable toxin
�to clear poison or fluid�
5. Dialysis (....diffusion) Solutes flow down an electrochemical gradient, across a membrane.
Solute removal is proportional to dialysate flow rate
Dialysate flows counter-current to blood
6. Ultrafiltration (..... convection) Water moves along a hydrostatic gradient across a filter
Solute moves by solvent drag
7. �There are no stupid questions, but there are a lot of inquisitive idiots�
Larry Kersten, American Sociologist
8. How can I dialyse a patient? Intermittent haemodialysis
Peritonal Dialysis
Rarely used in UK ICUs as labour intensive and risks infection, but nb CAPD
Continuous Haemodiafiltration
Arterio-venous (pts own BP drives blood through the filter)
Veno-venous (blood is pumped � doesn�t rely on BP)
Plasma exchange, esp in immune disorders, eg GBS
Plasma is removed / exchanged by filtration or centrifugation
9. Intermittent haemodialysis Gold standard � though patient must be haemodynamically stable
Dialysate is typically deionised water
Blood flow typically 200-400mL/min, dialysate flow 500mL/min, filtration rate of 300-2000mL/hr and urea clearance of 150/250mL/min
Complications mostly due to fluid and osmitic shifts
10. Problems with IHD Removal of intravascular volume quicker than it can be replaced from the extravascular space can cause cardiovascular collapse � particularly if intravascularly deplete.
Hypotension can cause ischaemic injury, particulary in AKI or head injury.
Intermittent by nature, so ICU patients may develop overload in-between sessions (nb reduced venous capacitance)
11. Dialysis Disequilibrium syndrome Self-limiting syndrome typically after first dialysis of very uraemic patients.
Characterised by nausea, vomiting, headache, seizures and coma.
Syndrome is triggered by rapid reduction in plasma osmolality causing cerebral (cellular) oedema.
Treatment
Supportive
Hypertonic saline / manitol
12. �Watson, you idiot. Somebody stole our tent.....�
Sherlock Holmes, Sleuth
13. Continuous veno-venous heamofiltration (CVVH) Convective dialysis
Filtration rate is high
Electrolyte replacement
solution is required
Removes a lot of middle
molecules, e.g. cytokines
Slow continuous ultra-filtration
(SCUF) is �slower� and doesn�t
use a replacement fluid
(i.e. removes volume
only)
14. Continuous veno-venous haemodialysis (CVVHD) Continuous diffusive dialysis
Mostly small molecules
are removed
15. Continuous veno-venous haematodiafiltration (CVVHDF) Diffusive and convective
dialysis
Small and middle
molecules removed
Requires dialysate and
replacement fluid
Most popular mode
16. �He is a dreamer, a thinker, a speculative philosopher... or, as I like to put it, an idiot�
Christina Hallsworth, my wife
17. Advantages of CRRT Suitable for use in haemodynamically unstable patients.
Precise volume control, which is immediately adaptable to changing circumstances.
Very effective control of uraemia, hypophosphataemia and hyperkalaemia.
Rapid control of metabolic acidosis
Available 24 hours a day with minimal training.
Safer for patients with brain injuries and cardiovascular disorders (particularly diuretic resistant CCF).
May have an effect as an adjuvant therapy in sepsis.
Probable advantage in terms of renal recovery
Makes space for TPN in anuria
18. Disadvantages of CRRT Expense � probably the same as IHD.
Anticoagulation � to prevent extracorporeal circuit from clotting.
Complications of line insertion and sepsis.
Risk of line disconnection.
Hypothermia.
Theraputic drugs doses need adjusting � nb vasoactive drugs
Severe depletion of electrolytes � particularly K+ and PO4, where care is not taken.
19. Using CVVHDF CVVHDF is similar to IHD � but in slow motion
Requires a 12F double lumen catheter (VasCath) in a big vein
Typically
Blood flow 100-200mL/min
Filtration rate 10-20mL/min
Urea clearance 10-20mL/min
To increase the urea clearance, you can increase the blood flow rate, dialysate flow rate, or both.
Membrane is usually a hollow fibre polyacrilonitrile, polyamide or polysulphone with a surface area of 0.6-1m2
20. Using CVVHDF Anticoagulation
Classically heparin, but :
Risks bleeding
Requires antithrombin 3
Causes HIT
PGI2 (prostacyclin � short t� ),
Citrate (binds Ca+, metabolised to bicarbonate in liver)
LMWH
Aprotonin
21. Using CVVHDF Typically the dialysate and replacement fluid are similar to �what you want the blood to be�, i.e. Hartmanns
Watch potassium, calcium and phosphate levels closely
There is often no bicarbonate in the dialysate, and bicarb in the blood is replaced with lactate from the dialysate.
This can be a problem in liver failure � best to use a lactate free dialysate
22. �When you left home you deprived the village of it�s idiot�
Chris Hallsworth, my father