Download
1 / 1
10 likes | 222 Views
AUDIT ON THE USE OF OXYTOCIN IN THE MANAGEMENT OF DELAY IN THE FIRST STAGE OF LABOUR Dr . MK Liew, T Oliver, Dr. D Basu University Hospital of North Tees, Stockton-on-Tees, England. BACKGROUND

E N D
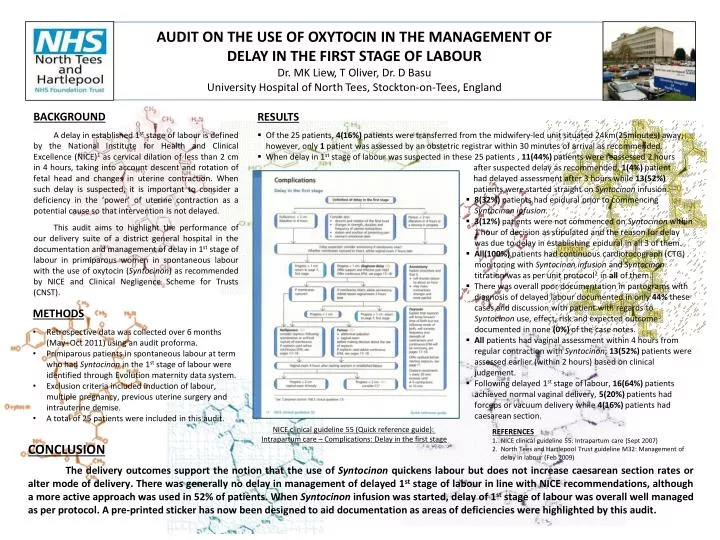
AUDIT ON THE USE OF OXYTOCIN IN THE MANAGEMENT OF DELAY IN THE FIRST STAGE OF LABOUR Dr. MK Liew, T Oliver, Dr. D Basu University Hospital of North Tees, Stockton-on-Tees, England BACKGROUND A delay in established 1ststage of labour is defined by the National Institute for Health and Clinical Excellence (NICE)1 as cervical dilation of less than 2 cm in 4 hours, taking into account descent and rotation of fetal head and changes in uterine contraction. When such delay is suspected, it is important to consider a deficiency in the ‘power’ of uterine contraction as a potential cause so that intervention is not delayed. This audit aims to highlight the performance of our delivery suite of a district general hospital in the documentation and management of delay in1st stage of labour in primiparous women in spontaneous labour with the use of oxytocin (Syntocinon) as recommended by NICE and Clinical Negligence Scheme for Trusts (CNST). • RESULTS • Of the 25 patients, 4(16%) patients were transferred from the midwifery-led unit situated 24km(25minutes) away, however, only 1 patient was assessed by an obstetric registrar within 30 minutes of arrival as recommended. • When delay in 1st stage of labour was suspected in these 25 patients , 11(44%)patients were reassessed 2 hours after suspected delay as recommended, 1(4%) patient had delayed assessment after 3 hours while 13(52%) patients were started straight on Syntocinoninfusion. • 8(32%) patients had epidural prior to commencing Syntocinon infusion. • 3(12%) patients were not commenced on Syntocinonwithin 1 hour of decision as stipulated and the reason for delay was due to delay in establishing epidural in all 3 of them. • All(100%) patients had continuous cardiotocograph (CTG) monitoring with Syntocinon infusionand Syntocinontitration was as per unit protocol2 in all of them. • There was overall poor documentation in partograms with diagnosis of delayed labour documented in only 44% these cases and discussion with patient with regards to Syntocinon use, effect, risk and expected outcome documented in none (0%) of the case notes. • All patients had vaginal assessment within 4 hours from regular contraction with Syntocinon; 13(52%) patients were assessed earlier (within 2 hours) based on clinical judgement. • Following delayed 1st stage of labour, 16(64%) patients achieved normal vaginal delivery, 5(20%) patients had forceps or vacuum delivery while 4(16%) patients had caesarean section. • METHODS • Retrospective data was collected over 6 months (May–Oct 2011) using an audit proforma. • Primiparous patients in spontaneous labour at term who had Syntocinonin the 1ststage of labour were identified through Evolution maternity data system. • Exclusion criteria included induction of labour, multiple pregnancy, previous uterine surgery and intrauterine demise. • A total of 25 patients were included in this audit. NICE clinical guideline 55 (Quick reference guide): Intrapartum care – Complications: Delay in the first stage REFERENCES NICE clinical guideline 55: Intrapartum care (Sept 2007) North Tees and Hartlepool Trust guideline M32: Management of delay in labour (Feb 2009) CONCLUSION The delivery outcomes support the notion that the use of Syntocinonquickens labour but does not increase caesarean section rates or alter mode of delivery. There was generally no delay in management of delayed 1st stage of labour in line with NICE recommendations, although a more active approach was used in 52% of patients. When Syntocinon infusion was started, delay of 1st stage of labour was overall well managed as per protocol. A pre-printed sticker has now been designed to aid documentation as areas of deficiencies were highlighted by this audit.