Download
1 / 30
350 likes | 754 Views
Medical Therapy of Prostate Symptoms (MTOPS). Jeannette Y. Lee, Ph.D. University of Alabama at Birmingham. Benign Prostatic Hyperplasia (BPH). Common cause of morbidity among older men Characterized by bothersome lower urinary tract symptoms (LUTS)

E N D
Medical Therapy of Prostate Symptoms (MTOPS) Jeannette Y. Lee, Ph.D. University of Alabama at Birmingham
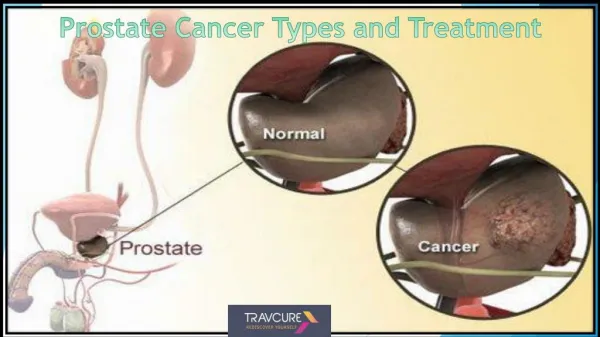
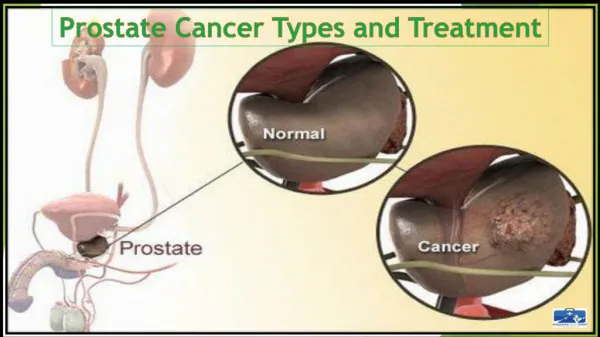
Benign Prostatic Hyperplasia (BPH) • Common cause of morbidity among older men • Characterized by bothersome lower urinary tract symptoms (LUTS) • Men with BPH and larger prostates due to BPH are at increased risk of complications such as acute urinary retention
Prevalence • Clinical Significant BPH • AUA symptom score > 7 points (moderate to severe lower urinary tract symptoms) • Depressed peak uroflow (< 15 mL/sec) • Prevalence by age group • 17% in men from 50-59 yrs of age • 27% in men from 60-69 yrs of age • 35% in men from 70-79 yrs of age
MTOPS Trial Design • Randomized, double blind, 2 x 2 factorial • Two-year enrollment period • Minimum four-year follow-up period • Objective: to determine if doxazosin or finasteride, alone or in combination delayed or prevented clinical progression of BPH
Inclusion Criteria • Men > 50 yrs of age • AUA symptom score of 8-35 • Peak urinary flow rate of 4-15 ml/sec • Voided volume > 15 ml
Exclusion Criteria • Prior medical or surgical intervention for BPH • Supine blood pressure < 90/70 mmHg • PSA > 10 ng/ml
Treatments • 5-areductase inhibitor Finasteride dose: 5 mg • Alpha blocker Doxazosin dose doubled weekly starting with 1 mg daily until daily dose of 8 mg reached.
Follow-up Evaluations • Vital signs • AUA symptom score • Urinary flow rate • Adverse Events • DRE, serum PSA< urinalysis • Prostate volume (TRUS)
Follow-up Questionnaire • AUA Symptom Score • QOL Short Form-36 (SF-36) • Sexual function questionnaire • Prostatitis Questionnaire
Primary Endpoints • Primary endpoint: time to BPH progression defined as • > 4 point increase in AUA symptom score • Acute urinary retention • Renal insufficiency • Recurrent urinary tract infection • Urinary incontinence
Secondary Endpoints • Changes over time • AUA symptom score • Maximal urinary flow rate • PSA level • Prostate volume • Cumulative incidence of invasive treatments for BPH
Results • 3047 men randomized • Baseline characteristics • Mean age: 62.6 yrs • White: 82% • Mean AUA symptom score: 16.9 • Mean prostate volume: 36.3 ml • Mean Max urinary flow rate: 10.5 ml/min • Mean post void residual volume: 68.1 ml • Mean serum PSA: 2.4 ng/ml • Mean serum creatinine: 1.1 mg/dl
Cumulative Incidence of Progression(N Engl J Med 2003: 349 (25): 2387-97)
Rate of Progression per 100 PYs • Placebo: 4.5 BPH Progressors • Doxazosin: 2.7 BPH Progressors • Finasteride: 2.9 BPH Progressors • Combination: 1.5 BPH Progressors
Adverse Events – Sexual Function(Rate per 100 PYs) * p<0.05 compared to placebo
Adverse Events – Hypotension(Rate per 100 PYs) * p<0.05 compared to placebo
MTOPS Summary • Combination therapy with doxazosin and finasteride was safe and reduced the risk of overall clinical progression more than each drug alone. • Finasteride containing regimens reduced the long-term risk of AUR and need for invasive therapy. McConnell et al, N Engl J Med 2003.
Methods papers • Study Design • Bautista et al, Controlled Clinical Trials 2003 • Recruitment • Kusek et al, Controlled Clinical Trials 2002
Secondary Analyses • Placebo patients – baseline factors associated with clinical progression * • Total prostate volume • PSA • Peak flow rate • Post residual volume • Age * Crawford et al, J Urol 2006
Secondary Analyses • Combination therapy is better than either agent alone (finasteride, doxazosin) in decreasing the risk of clinical BPH progression in those with higher prostate volumes* Kaplan et al, J Urol 2006
MPSA • MTOPS Prostatic Sample Analysis Consortium – evaluate biomarkers associated with BPH (Mullins et al, J Urol 2008).
Analyses in Progress • Longitudinal analyses of sexual function • Risk of prostate cancer
MTOPS Data Available • Uroflow Measurements (quarterly) • Compliance/pill counts (quarterly) • PSA measurements (semi-annually) • PE, CBC, serum chemistry, urinalysis (annually) • TRUS and Biopsy (Screening, 12 mos, end of study)
MTOPS Questionnaires • AUA Symptom Questionnaire (quarterly) • Sexual Function Questionnaire (screening and end of study) • Medical Outcomes Study (MOS) – Short Form 36 (SF-36) (annually) • Prostatitis Questionnaire (annually)
MTOPS Data from Diagnostic Center • PSA (ng/ml) • LH (mIU/ml) • Testosterone (ng/dl) • % Free PSA • Total PSA