Download
1 / 32
730 likes | 1.9k Views
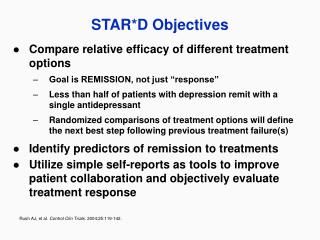
STAR*D: Lessons for us all ?. Prof Yoram Barak, MD, MHA. and Shelly Tadjer, MD. Abarbanel M.H.C. and the Sackler School of Medicine, Tel-Aviv University. CATIE-Sciz CATIE-AD. STEP-BD STAR*D. The “ Big-4 ”.

E N D
STAR*D:Lessons for us all ? Prof Yoram Barak,MD, MHA. and Shelly Tadjer, MD. Abarbanel M.H.C. and the Sackler School of Medicine, Tel-Aviv University. Prof Y Barak
CATIE-Sciz CATIE-AD STEP-BD STAR*D The “Big-4” Prof Y Barak
Schizophr Bull. 2003;29(1):15-31The National Institute of Mental Health Clinical Antipsychotic Trials of Intervention Effectiveness (CATIE) project: schizophrenia trial designand protocol development .Stroup TS, McEvoy JP, Swartz MS, Byerly MJ, Glick ID, Canive JM, McGee MF, Simpson GM, Stevens MC, Lieberman JA. Prof Y Barak
Am J Geriatr Psychiatry. 2001 Fall;9(4):346-60.National Institute of Mental Health Clinical Antipsychotic Trials of Intervention Effectiveness (CATIE): Alzheimer disease trial methodology.Schneider LS, Tariot PN, Lyketsos CG, Dagerman KS, Davis KL, Davis S, Hsiao JK, Jeste DV, Katz IR, Olin JT, Pollock BG, Rabins PV, Rosenheck RA, Small GW, Lebowitz B, Lieberman JA. Prof Y Barak
Biol Psychiatry. 2003 Jun 1;53(11):1028-42Rationale, design, and methods of the systematic treatment enhancement program for bipolar disorder (STEP-BD).Sachs GS, Thase ME, Otto MW, Bauer M, Miklowitz D, Wisniewski SR, Lavori P, Lebowitz B, Rudorfer M, Frank E, Nierenberg AA, Fava M, Bowden C, Ketter T, Marangell L, Calabrese J, Kupfer D, Rosenbaum JF. Prof Y Barak
STAR*D Treatment Trial for Depression STAR*D (Sequenced Treatment Alternatives to Relieve Depression) is a multisite, prospective, sequentially randomized controlled trial of outpatients with nonpsychotic major depressive disorder that is using randomization to compare various switching or augmenting strategies either commonly used or that are based on pharmacologic reasoning. The study includes self-declared patients seeking treatment at either primary or specialty care practices. Prof Y Barak
STAR*D Background Major depressive disorder is a common, costly, and disabling condition affecting 4.9%–17.9% of the population in a lifetime. From 20%–30% of affected persons suffer a chronic, relapsing course. Many medications and several time-limited psychotherapies have shown established efficacy in randomized controlled trials. Among outpatients with major depressive disorder treated for the first time, about 50% will have a response (i.e., exhibit a clinically significant symptom reduction). However, of these “responders,” only 50%–70% will achieve symptom remission, which, since remission is associated with the best day-to-day functioning and best prognosis, is the goal of treatment. Prof Y Barak
STAR*D Rationale For those cases of depression not remitting with the first treatment, little controlled trial evidence is available by which to select the next treatment. It is believed that a switch to a new, second treatment may result in a 50% response rate, with lower response rates expected with the third or fourth treatment step. Psychiatry faces the challenge of recommending the next best treatment steps, or series of steps, for depressed persons not experiencing a remission with the first or subsequent treatments. Therapeutic strategies may include switching (i.e., stopping one treatment and starting another) or augmenting/combining (i.e., adding a second treatment to the first). Prof Y Barak
STAR*D Design Patients, as in practice, may select among the strategies. For instance, a patient may choose to only accept augmentation or only switching. However, all participants are randomly assigned to the specific treatments within the strategies that they find acceptable. This so-called equipoise stratified randomized design mimics clinical practice, so that results should have high practical relevance. Prof Y Barak
STAR*D The Promise:Am J Psychiatry 160:2, February 2003 Response, remission, daily functioning, and service cost/utilization will be objectively assessed. Results, expected in the year 2006, will determine whether there is a preferred next step for varying types and degrees of treatment-resistant depression. A. JOHN RUSH, M.D. MADHUKAR TRIVEDI, M.D. Dallas, Tex. MAURIZIO FAVA, M.D. Boston, Mass. Prof Y Barak
STAR*D Data:60 publications, 3 reviews. • Trivedi et al. Maximizing the Adequacy of Medication Treatment in Controlled Trials and Clinical Practice: STAR(*)D Measurement-Based Care. Neuropsychopharmacology. 2007 April • Fava et al. Background and rationale for the sequenced treatment alternatives to relieve depression (STAR*D) study. Psychiatr Clin North Am. 2003 June Prof Y Barak
Evaluation of Outcomes With Citalopram for DepressionUsing Measurement-Based Care in STAR*D:Implications for Clinical PracticeAm J Psychiatry 2006; 163:28–40 Method: This clinical study included outpatients with major depressive disorder who were treated in 23 psychiatric and 18 primary care “real world” settings. The patients received flexible doses of citalopram prescribed by clinicians for up to 14 weeks. The clinicians were assisted by a clinical research coordinator in the application of measurement-based care, which included the routine measurement of symptoms and side effects at each treatment visit and the use of a treatment manual that described when and how to modify medication doses based on these measures. Remission was defined as an exit score of ≤7 on the 17-item Hamilton Depression Rating Scale (HAM-D) (primary outcome) or a score of ≤5 on the 16-item Quick Inventory of Depressive Symptomatology, Self-Report (QIDS-SR) (secondary outcome). Response was defined as a reduction of ≥50% in baseline QIDS-SR score. Prof Y Barak
STAR*D Step 1 Results Nearly 80% of the 2,876 outpatients in the analyzed sample had chronic or recurrent major depression; most also had a number of comorbid general medical and psychiatric conditions. The mean exit citalopram dose was 41.8 mg/day. Remission rates were 28% (HAM-D) and 33% (QIDS-SR). The response rate was 47% (QIDS-SR). Patients in primary and psychiatric care settings did not differ in remission or response rates. A substantial portion of participants who achieved either response or remission at study exit did so at or after 8 weeks of treatment. Participants who were Caucasian, female, employed, or had higher levels of education or income had higher HAM-D remission rates. Longer index episodes, more concurrent psychiatric disorders (especially anxiety disorders or drug abuse), more general medical disorders, and lower baseline function and quality of life were associated with lower HAM-D remission rates. Prof Y Barak
29.7 % of Eligible subjects Prof Y Barak
LEVEL 2: SWITCH TO: bupropion (sustained-release), cognitive therapy, sertraline, venlafaxine XR OR AUGMENT WITH: bupropion SR, buspirone, cognitive therapy AUGMENT: Citalopram MFD: 55 mg SWITCH Bupropion Max Dose 400 N=239 Bupropion Max Dose 400 N=565 Buspirone Max Dose 60 N=286 21.3% Sertraline Max Dose 200 N=238 29.7% 30.1% 17.6% Venlafaxine Max Dose 375 N=250 24.8% Prof Y Barak
LEVEL 3: SWITCH TO: mirtazapine or nortriptyline OR AUGMENT WITH: lithiumor T3 SWITCH AUGMENT: Antidepressant from level 2 Mirtazapine Max Dose 60 N=114 Lithium Max Dose 900 N=69 T3 Max Dose 50mcg N=73 12.3% Nortriptyline Max Dose 200 N=121 15.9% 24.7% 19.8% Prof Y Barak
LEVEL4: SWITCH TO: tranylcypromine or mirtazapine combined with venlafaxine XR SWITCH Mirtazapine + Venlafaxine Max Dose 35.7 +225 N=51 Tranylcypromine Max Dose 36.9 N=58 13.7% 6.9% Prof Y Barak
Editorial: J. CRAIG NELSON, M.D.Am J Psychiatry 163:11, November 2006The STAR*D Study: A Four-Course Meal ThatLeaves Us Wanting More The STAR*D study is the largest prospective study of a sequential series of treatments for depression ever conducted. In this study, 3,671 patients entered treatment at 41 sites, 18 of which were primary care facilities. Inclusion criteria were generous. Of the patients entering the first treatment step, 61.5% had a concurrent psychiatric disorder. As the result of broad inclusion criteria, the STAR*D study is more representative of patients in clinical practice. Prof Y Barak
The STAR*D Study: A Four-Course Meal ThatLeaves Us Wanting MoreRemission The study confirms that about one-third of patients achieve remission with initial treatment and that remission rates decline with successive treatment failures. Remission rates were 36.8%, 30.6%, 13.7%, and 13% after treatment steps 1 through 4. The authors note that remission rates drop more substantially after two failed treatments. This might support the developing notion that treatment-resistant depression is defined by two prior treatment failures. Prof Y Barak
The STAR*D Study: A Four-Course Meal ThatLeaves Us Wanting MoreRelapse Consistent with prior data, patients who achieve remission are less likely to relapse than patients who have only responded. Rates of relapse ascend with each treatment step. Among those achieving remission, relapse rates were 33.5%, 47.4%, 42.9%, and 50.0% after the four treatment steps. Relapse rates were even higher in patients who improved but did not achieve remission (range=59% to 83%). Prof Y Barak
The STAR*D Study: A Four-Course Meal ThatLeaves Us Wanting MoreDrop-out The study also found that intolerance increased after each treatment step: 16.3%, 19.5%, 25.6%, and 34.1%. Readers should remember that the term “intolerance” includes dropouts for any reason during the first 4 weeks, or side effects after that. One might expect that side effect rates would decline with each step (once those prone to side effects drop out). Perhaps patients that drop out are becoming demoralized with each failure and are giving up. Prof Y Barak
The STAR*D Study: A Four-Course Meal ThatLeaves Us Wanting More“Positive side…” In my opinion, the authors have cited the positive side of the coin here. They note that after four treatments the cumulative remission rate is 67%. But this does not account for relapse. If the goal of treatment is sustained recovery, relapse should be considered. I found a cumulative sustained recovery rate of 43% after four treatments, using a method similar to the authors but taking relapse rates into account. Prof Y Barak
The STAR*D Study: A Four-Course Meal ThatLeaves Us Wanting More“Worrisome…” It is particularly worrisome that at steps 3 and 4, in addition to low remission rates (13.7% and 13.0%), nearly half of those remitting relapsed. Treatment in the relapse phase was naturalistic: patients were encouraged to remain on their last treatment, but treatment changes or other treatments were allowed. But regardless of that, from step 2 on, less than half of those responding and remitting remained well. Prof Y Barak
The STAR*D Study: A Four-Course Meal ThatLeaves Us Wanting MoreRandomization The greatest disappointment of the study — depending on your perspective — was that patients were not randomly assigned to all treatments at level 2, and as a result comparisons between treatment strategies were limited. Patients were given the option of declining or accepting certain treatments. Patients who agreed to augmentation or switching strategies were randomly assigned within those groups. The authors decided on this design to mimic real practice and to improve recruitment and retention. They discovered, however, that patients have their own opinions. Only 21 of 1,439 patients (1.5%) agreed to randomization to all of the treatment choices at level 2. As a consequence, it is not possible to compare augmentation with switching or with cognitive therapy. Prof Y Barak
The STAR*D Study: A Four-Course Meal ThatLeaves Us Wanting MoreComparing strategies One of the surprises of the study was the finding that among patients who switched to another drug, a second SSRI (sertraline) was just as effective as a drug with a different mechanism (bupropion) or a “dual-action” agent (venlafaxine). Does this mean longer duration is just as important as the drug chosen? This study was not placebo controlled, and it is not possible to determine what portion of response was associated with nonspecific factors (which would tend to obscure true drug differences). Regardless of these limitations, this study remains the largest to randomize and compare three switches after a prospectively documented treatment failure. While treatment was open label, the expected bias would seem to favor bupropion or venlafaxine. The findings challenge commonly held beliefs. Prof Y Barak
The STAR*D Study: A Four-Course Meal ThatLeaves Us Wanting MoreThe future… The STAR*D study provides a wealth of data about treatment of depression. It offers hope to patients that successive treatments will increase their chance for remission. Overall, the study provides “benchmarks” for the field in terms of the effectiveness of current treatments for depression. Yet the relapse data are sobering. The lack of difference between switching strategies at level 2 will no doubt stimulate much debate. Perhaps most disconcerting, the lack of differences between treatments at levels 2, 3, and 4 leaves us without a roadmap to guide treatment selection and leaves us wanting more. Prof Y Barak
Thank you for your attention ! Prof Y Barak