Download
1 / 107
1.14k likes | 1.54k Views
Approach to TIA and Management of Stroke after 4.5 hours. Robert Altman R4 McGill University August 25 th 2010 Summer Emergency Lecture Series. What to take out of today. Everything I’m presenting is evidence based Where no data or consensus exists, will have to resort to ‘expert opinion’

E N D
Approach to TIA and Management of Stroke after 4.5 hours Robert Altman R4 McGill University August 25th 2010 Summer Emergency Lecture Series
What to take out of today. • Everything I’m presenting is evidence based • Where no data or consensus exists, will have to resort to ‘expert opinion’ • Tried to make this as user friendly and practical so as to be able to refer back to at a future date • Basic standards of practice • know the guidelines, or where to find them; especially the Canadian ones. • Know the terminology and classification systems that exist to facilitate your readings and assist in critically appraising studies.
Outline • Definition • TIA • Ddx and TIA mimics • Review of ABCD2 score • 48 hr cerebrovascular risk stratification • Who to admit and who can be discharged • Subacute management of ischaemic arterial stroke (and TIA for that matter) • Practical aspects and highlights of frequently cited studies • Topics: CEA, BP, lipids, oxygenation, mobilization, swallowing, speech, VTE prophylaxis Next week...
TIA • Old definition • “Sudden, focal neurological deficit of presumed vascular origin lasting ≤ 24 hours” • Suggests transient ischemic symptoms are benign • Diagnosis on the basis of temporal course rather than pathophysiological basis (tissue) • Delays and obfuscates diagnosis • Delays intervention in cases of true brain ischemia • Diverges from the notion that TIA is to stroke what angina is the MI
History • 24-hour threshold arose in the mid-1960s. • Assumption was that no permanent brain injury if symptoms dissipated. • Reversible ischemic neurological deficit (RIND) was applied to events lasting 24 hours to 7 days. • >7 days indicate infarction and received the designation stroke • 1970s • Great preponderance of events lasting 24hrs-7d were a/w infarction, rendering the RIND obsolete • More recently, Hi-Res CT and diffusion-weighted MR studies demonstrate symptoms lasting 24 hours also are associated with new infarction. • 30% to 50% of classically defined TIAs show brain injury on diffusion-weighted magnetic resonance (MR) imaging (MRI) • These findings highlight an inconsistency between the concept of TIA (ischemia causing symptoms but no infarction) and the traditional definition of TIA
Transient Ischemic Attack • Tides have turned • Time (old) vs. Tissue based definition (new) • AHA/ASA 2009 definition • “Transient ischemic attack (TIA): a transient episode of neurological dysfunction caused by focal brain, spinal cord, or retinal ischemia, without acute infarction.” • No infarction on MRI • ‘acute neurovascular syndrome’ if no imaging available N Engl J Med, Vol. 347, No. 21
Transient Ischemic Attack • Diagnostic certainty will depend on the extent of evaluation the individual patient receives. • This concept is not unique to brain ischemia; it is typical of most medical diagnoses. • Brain imaging currently and serum diagnostic studies likely in the future (equivalent to trops) increase diagnostic certainty regarding whether a particular episode of focal ischemic deficits was a TIA or a cerebral infarction.
TIA • TIA is a very serious warning sign • Among patients presenting to the ER with a TIA • 10 to 15% of patients have a stroke within 3 months • halfoccurring within 48 hours • When recurrent TIAs, myocardial infarction and death from any cause are considered, the risk is more than 25% over the first 3 months. • Mortality • 5-6 % annually, mainly by MI Early recognition of TIA and subsequent timely intervention is of critical and obvious importance.
TIA Risk Gladstone D et al. CMAJ. 2004 Mar 30;170(7):1099-104.
Epidemiology • In the US, incidence is approx. 200 000 to 500 000 per year, with a population prevalence of 2.3% that translates into 5 million individuals • Lack of recognition by both the public and healthcare systems (including physicians), thus current #’s: • grossly underestimated
Signs / Symptoms • Neurological • Focal • Sudden • Localizable to an anatomical structure in the CNS or retina
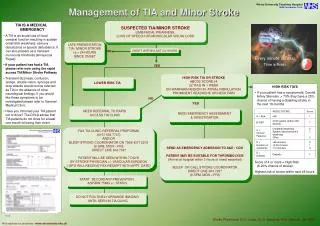
Immediate Management • Get a real history • Carefully examine the patient for residual deficits and try to localize anatomically to guide your work-up • Construct a differential diagnosis based on history • Recognize the mimics
TIA/Stroke Mimics CMAJ 2004;170(7):1134-7
Example: Real case • 76F remote CVA, 6 months prior, R MCA territory, near full recovery • Husband heard thump on the floor this AM 10:30, now 12:00 • Went to see wife, panicked, unresponsive, called ambulance. Ambulance note states pt had urinary incontinence (new) • In ER, staff notes patient was awake, but not really responding to commands, then eyes began deviating L then became obtunded and comatose. • Intubated • Exam shows flaccid plegia on L, minimal to no response to pain, withdraws, varying degrees on R. Both plantarsupgoing. CT head shows nil acute, old R MCA infarct. • What is going on here? • Is this a TIA/Stroke? NO
Example #2 • 36 M • Hx of paranoid schizophrenia, morbidly obese, HTN, dyslipidemia, and CAD with angina • Called for code stroke • Patient’s neck forced into sideflexion, mouth an tongue stuck open, unable to speak but follows commands well, no obvious other neurologic deficits. • What’s going on? • Is this a TIA/Stroke? NO
Example #3 • Mr. P, a 76-year-old man, presents to the emergency department after experiencing a sudden onset of slurred speech associated with tingling and clumsiness of his right hand. • Symptoms lasted about 30 minutes and have completely resolved. • His examination is now unremarkable. • He has a history of hypertension (controlled on medication) and dyslipidemia. • What’s going on? • Is this a TIA/Stroke? Indeed
Triage – Risk Stratification • Establishes who you will admit for expedited work-up • What is the critical information to garner from a TIA evaluation • Age, sex • PmHx: afib or PAF, prior TIA or CVA, CAD or recent MI, smoker, famHx of premature CVA • Symptoms: only motor, sensory, speech or both • BP and ECG rythm • Total duration of symptoms (5 min?, 25 min? 24 hrs?) • When? (today, yesterday, 6 months ago?)
=ABCD2 Lancet 2007; 370: 1432–42
Concentrate on duration, focality to weakness, DM and BP Lancet 2007; 370: 1432–42
Express • Phase 1 vs. 2 • Expedited medical and surgical management rather than give recommendations to primary care practitioner • Conclusion: Urgent assessment and early initiation of a combination of existing preventive treatments can reduce the risk of early recurrent stroke after TIA or minor stroke by about 80%, and reduce the total number of all early recurrent strokes in the whole population by over half Rothwell et al. Lancet 2007; 370: 1432–42
Cumulative proportions of patients prescribed new medication Statin Clopidogrel 1 anti-HTN Rx 2 anti-HTN Rx’s Lancet. 2007 Oct 20;370(9596):1432-42
FYI • TOAST classification system • Acute and preventive treatments can and should be tailored to the underlying mechanism implicated. Stroke 1993;24;35-41
What is an expedited work-up? (AHA, CSC) *local strengths in that expertise in vascular imaging dictate what to select as first line (also other medical conditions i.e. PM or RF) • Neuroimaging • MRI with DWI, PWI • CT (C-) • Vascular imaging (extracranial & intracranial)* • CUS • CTA (results comparable to CUS and MRA). • NPV of excluding >70% carotid stenosis of 100% • MRA (2D TOF) or MRA with contrast (superior resolution– has even supplanted catheter angiography in some centers, but limited utility if renal disease) • TCD (microembolic signals) • Conventional angiography • Cardiac and ‘other’ testing • ECG (r/o afib, SSS, arrythmia, LVH) • TTE, TEE • Holter • Routine bloodwork • CBC, SMA7, Coags, E+, FLP, CK, LFT’s • Hypercoagulable work-up depending on age / cryptogenicity of stroke-TIA
Clinical Case • Sudden onset dysarthria, mild R hemiparesis after a fall, or was it before the fall? • 60 min ago • Would you give this pt clopidogrel?
Sudden onset • Focal L hemiparesis • Dysarthria • 45 min ago • Anti-platelet?
Canadian Stroke Strategy • Carotid imaging should be performed within 24 hours of a carotid territory transient ischemic attack or nondisabling ischemic stroke (if not done as part of the original assessment) unless the patient is clearly not a candidate for carotid endarterectomy [Evidence Level B]
What about the echo? (AHA, CSC) • Should you hold the patient overnight for an echo? • “TIAs require urgent evaluation, but there is little evidence that early echocardiographic evaluation has a higher yield.” • The echocardiographic method used is important. • TEE is more sensitive than TTE for atheroma of the aortic arch and abnormalities of the interatrial septum (eg, atrialseptal aneurysm, PFO, atrialseptal defect), atrial thrombi, and valvular disease. • Holter monitoring is abnormal in a minority of unselected patients with TIA. • However, prolonged cardiac monitoring (inpatient telemetry or Holter monitor) is useful in patients with an unclear origin after initial evaluation. • The longer you can obtain the better
TIA Prognosis (summary) Timing weeks ago hours ago Duration sec – few minutes >10 min Frequency multiple one to few Sensory yes alone no Motor no yes Speech no yes Risk factors no HTN, DM, Deficit dynamics Mild at onsetSevere at onset Benign Malignant
What are the other modifiable cerebrovascular risk factors? Part 2 Treatment of acute stroke after 4.5 hrs
Drowning in a Sea of Strokes • Dr. Charles Miller Fisher • House officers and students learn neurology “stroke by stroke” • >50% of neurological admissions • 50,000 new /year in Canada • 3rd most important cause of death • after heart disease and cancer • Most important cause of adult disability • 30% of survivors require daily assistance.
Clinical Presentation • Sudden • Focal weakness, language impairment, gaze deviation, hemianopia • Neuroanatomically based • Search for warning symptoms in week prior • Amaurosisfugax • Sentinel TIA’s
Modifiable Risk Factors for Ischemic Stroke Sacco R. In Gorelick P, Alber M. handbook of Neuroepidemiology, New York, NY, Marcel Dekker Inc, 1994:77-19
High Blood Pressure • The most important modifiable risk factor (2-5 x) • Ischemic (primary and secondary), bleeding, “silent strokes” • Contributes to: • Large-vessel atherosclerotic disease • Small-vessel (lacunar) disease • LV dysfunction and Afib • Untreated HTN increases stroke risk 3-4 times. Treatment can reduce stroke risk and fatalities ~40%. • Most patients require 2 or more agents • CHEP guidelines • <140/90 (or if diabetes <130/80)
Acute BP Therapy •Randomized controlled trials have not defined the optimal time to initiate blood pressure lowering therapy after stroke or transient ischemic attack. •It is recommended that blood pressure lowering treatment be initiated (or modified) prior to discharge from hospital. • For patients with nondisabling stroke TIA not requiring hospitalization, blood pressure lowering treatment should be initiated (or modified) at the time of the first medical assessment
Acute Hypertension Management • AHA guidelines • Lower only if > 220/120 mmHg • or 185/110 for rt-PA • Labetalol 10-20 mg IV q 10-20 min (or nitroprusside infusion) • Goal is 15-25% reduction within first 24hrs Adams et al. Guidelines for the early management of adults with ischemic stroke. A guideline from the AHA/ASA stroke council… Stroke 2007;38:1655-1711.
Acute Hypertension Management • But remember, impaired auto-regulation is relative • If I’ve been walking around for 5 yrs with a BP 210/140, be careful about dropping it too much • Your ischemic penumbra is depending on that pressure • Use the AHA 15% rule!
Pathophysiology Ischemic PENUMBRA • Metabolically active tissue • 15-20% CO • Complete arrest of flow: • 15 sec: suppression of electric activity • 2-4 min: inhibition of synaptic excitability • 4-6 min: inhibition of electric excitability • Normal CBF > 55ml/min/100 g • CBF<18 ml/min/100 g: electric failure • CBF < 8 ml/min/100g: membrane failure