Download
1 / 1
20 likes | 204 Views
Pulmonary Paragonimiasis Mimicking Tuberculosis in a Middle-Aged Burmese Female. Amjad Ali, MD¹ , Allen T. Griffin, MD,¹ Hanan Farghaly, MD,² and Forest W. Arnold, DO, Msc¹

E N D
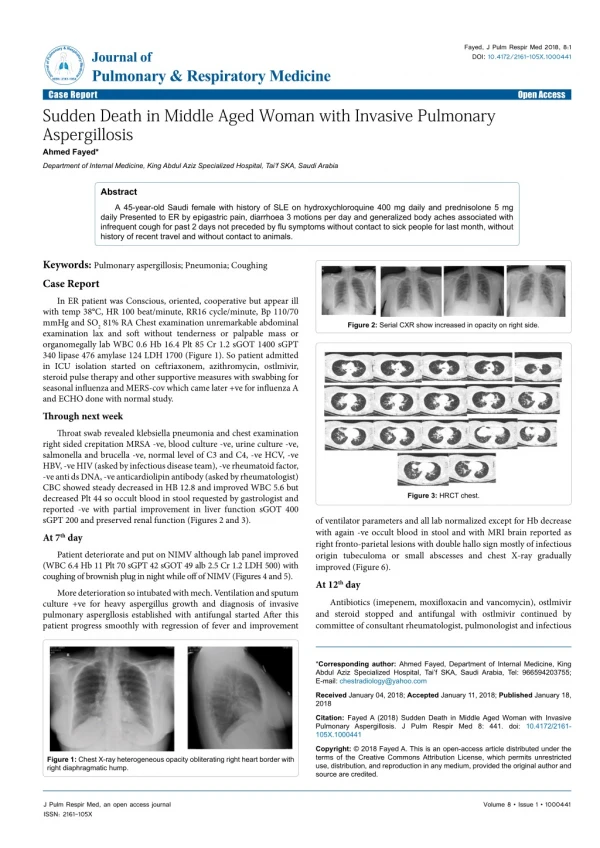
Pulmonary Paragonimiasis Mimicking Tuberculosis in a Middle-Aged Burmese Female. Amjad Ali, MD¹ , Allen T. Griffin, MD,¹ Hanan Farghaly, MD,² and Forest W. Arnold, DO, Msc¹ 1Division of Infectious Diseases, University of Louisville.2Department of Pathology, University of Louisville , Louisville, KY DISCUSSIONS (Cont’d) CASE REPORT (Cont’d) BACKGROUND CASE REPORT (Cont’d) The patient had a negative enzyme-linked immunoabsorbent assay (ELISA) for human immunodeficiency virus and a negative QuantiFERON® TB Gold (Cellestis, Ltd., Carnegie, Australia). Chest roentgenogram revealed a right lower lobe infiltrate that corresponded to an ovoid area of mass-like consolidation on computed tomography (CT) in the right lower lobe measuring 5.3 cm x 3.2 cm in greatest transverse diameter and approximately 5.8 cm craniocaudal with suspicion of early cavitation (Fig. 1). Mediastinal and hilar lymphadenopathy were noted as was a partially calcified linear lesion emanating from the diaphragm (Fig. 2). The patient was suspected to have a subacute community-acquired pneumonia (CAP). She was felt unlikely to be infected with organisms causing acute CAP; therefore, antibiotics were not initiated. The predominant differential diagnostic considerations were tuberculosis, non-tuberculous mycobacteria, Nocardia or Actinomycesinfection, or less likely an endemic fungal infection contracted in the United States or Burma. Sputum was induced to ascertain the etiology of her illness. Stains for acid fast bacilli and fungi were negative, as were cultures for these organisms. Standard bacterial cultures yielded normal flora. A CT-guided lung biopsy was pursued for definitive diagnosis, and the biopsied tissue was submitted for microscopic evaluation as well as cultures. Pathologic examination of the biopsied tissue revealed scattered eggs embedded in the lung parenchyma, producing an eosinophil-rich, dense inflammatory reaction with nodular granulomatous lesions. The visualized eggs [90-100 µm x 50-60 µm (length x width)] were ovoid and contained exudate and debris (Fig. 3A). A Paragonimus parasitic infection was suspected morphologically and was further supported using a polarized lens. The visualized eggs were birefringent under polarized light, a distinctive characteristic of Paragonimus species (Fig. 3B). Polymerase chain reaction testing for unequivocal species identification was not undertaken, and details of ova morphology were partially distorted on processing. However, based on the size of the ova and suspected region of acquisition, Paragonimus westermani was thought to be the etiology in this instance. Special stains were performed on the lung biopsy for acid fast bacilli and fungi; these stains, as well as cultures performed for these organisms, were all negative. As the diagnosis was secured pathologically, serology for Paragonimus was not procured. Given the diagnosis of paragonimiasis, the patient was treated with praziquantel at 25 mg/kg three times per day for two days and discharged from the hospital. She was followed in clinic within one month, and she reported a demonstrable improvement in symptoms Paragonimiasis is a food-borne parasitic infection resulting from ingestion of undercooked crustaceans. While uncommon in the United States, Paragonimus species are endemic in North America, South America, Asia, and Africa. Pulmonary symptoms are most common, but cerebral, dermatologic, and abdominal variations are recognized. Diagnosis is supported by positive serology and a typical exposure history. Pathologic confirmation by visualization of eggs, however, is preferred. In the subsequent case presentation, we elucidate an instance of pulmonary paragonimiasis mimicking tuberculosis in a middle-aged Burmese female A 51-year-old Burmese female was admitted to the hospital for cough and hemoptysis. She relayed a history of hyperlipidemia and mild chronic-obstructive pulmonary disease (COPD), but was otherwise healthy. Upon her current hospital presentation, she described having a non-productive cough intermittently for two years, which had been attributed to COPD. However, during the past month, the cough had become more forceful with production of sputum and blood. She could not recall specific circumstances that exacerbated the cough and noted no post-tussive emesis. Associated signs and symptoms of the current illness included night sweats, shortness of breath on exertion, malaise, periodic fevers to 101°F, and weight loss of 10 pounds in the previous month. On one occasion since becoming ill, the patient had been diagnosed with bronchitis by her primary care physician and treated with doxycycline, but her symptoms did not abate. On the day of hospital admission, she was brought to the emergency room after an episode of syncope associated with coughing. The patient was being treated with low-dose inhaled corticosteroids for COPD associated with smoking and baclofen for intermittent muscle spasms. She reported no medication allergies. Past surgeries included a tubal ligation 13 years earlier. She was a 30 pack year smoker, but consumed no alcohol or illicit drugs. She resided in the city of Louisville, Kentucky, with her two teen-age children as well as three other adults from Burma. The patient worked in a laundromat and immigrated from Burma three years prior; however, she would occasionally return to her home country to visit family where she would consume uncooked, freshwater crustaceans, including crayfish and crab. Although she was not certain, she could not recall direct exposure to individuals with tuberculosis and had never been incarcerated. On physical examination, the patient was alert, but appeared uncomfortable. Her temperature was 98.0° F, pulse 61 beats per minute, blood pressure 117/72 mm of Hg, and respiratory rate 16 breaths per minute. Oxygen saturation was 98 % on ambient air. The oral mucosa was dry, but revealed no lesions or thrush. There was no cervical, supraclavicular, axillary, or inguinal lymphadenopathy. The cardiac exam was without murmurs. Diffuse wheezing was detected on the pulmonary exam with focal rales in the right lower lung zones noted. The remainder of the physical exam was unremarkable. Laboratory findings, including a complete blood count and complete metabolic panel, were unrevealing, with the exception of a slight eosinophilia of 9 % and an erythrocyte sedimentation rate of 66 mm/hour (Table 1). . Although an ELISA is available through the Centers for Disease Control and Prevention,14 confirmation of disease by visualization of ova or adult worms is preferential. Adult worms are infrequently identified in patient specimens; however, if present, the adults are distinctively large and contain a conspicuous cuticular spine.1 For lung parenchymal involvement, acid-fast stains15 and standard ova and parasite examinations of sputum may reveal diagnostic ova, but these techniques are insensitive. Specimens procured by bronchoscopy with biopsy or other means are more sensitive and may reveal large parasite ova (60-120µm)1 in addition to eosinophilic infiltration and possibly granulomas in biopsy specimens.16 Ova may be particularly difficult to locate in the event of a pleural effusion with no parenchymal involvement. In such cases, a careful epidemiologic history and serology are most useful, as pleural fluid eosinophilia is an inconstant and non-specific finding.6 Serology may also be of use in other instances in which pathologic samples are nondiagnostic or when sensitive areas, such as the eye or brainstem, would have to be biopsied to attain a pathologic diagnosis.Ova from Paragonimus species can be discerned from related genera such as Schistosoma by birefringence under polarized light, as in the current case (Fig. 3B), and the presence of an operculum. Cytologic, in contrast to histologic, analysis may be most beneficial in equivocal cases, as ova morphology is less likely to be compromised.1 The best studied antihelminthics for this disease are praziquantel18 and triclabendazole.19Triclabendazole is not available in the United States; therefore, the recommended regimen in the Unites States is praziquantel given as 25 mg/kg orally three times per day for two days. Figure 3: Paragonimus egg embedded within a granulomatous inflammation, 40X (Fig. 3A). The polarized lens highlights the Paragonimus egg’s refractile wall, 40 X (Fig. 3B). Eggs are 95 µm x 55 µm (length x width). CASE REPORT DISCUSSIONS TheParagonimus genus is of the Trematode class within the phylum Platyhelminthes and, thus, is closely related to the schistosomes. While the Paragonimus genus may contain nearly 40 distinct species, only a few are routinely found in man, the most common of which worldwide is Paragonimus westermani (P. westermani). Regional differences exist with respect to the species routinely encountered, with the most frequently diagnosed in indigenous cases in the United States being Paragonimus kellicotti (P. kellicotti).1 Paragonimus species are found in Asia, Africa, and North and South America.1 The propensity to acquire the disease is less a function of endemicity than regional dietary customs. Eggs released from mammalian hosts typically hatch and mature into miracidia that are ingested by mollusks such as snails. Within the snail, the miracidia eventually mature into cercariae. Subsequently, when the snail is consumed by a crustacean, cercariae are released and encyst in the crustacean as metacercariae. Upon consumption of the crustacean by a mammal, metacercariaeexcyst, penetrate the duodenum of the mammalian host, travel through the peritoneal cavity, and cross the diaphragm to encyst in the lungs where they mature into adults.2 Thus, consumption of uncooked crustaceans, crayfish3 or freshwater crabs,4 a more common practice in Asia and Africa, results in paragonimiasis. The signs and symptoms of paragonimiasis are usually pulmonary, as metacercariae typically encyst and mature into adults in the lungs. The typical presentation involves cough and hemoptysis with the variable presence of fever and other systemic complaints;5 however, if infection is limited to the pleura, hemoptysis and cough can be absent, and pleuritic chest pain may dominate the clinical picture.6 Elevated levels of blood eosinophils and immunoglobulin E, though common, are not invariably present.1 While pleural effusions,6 pneumothoraces,7 and chylothoraces8 have all been noted, the most common radiologic features are cystic pulmonary lesions, nodules, or cavitary lung lesions.8,9 Linear opacities representative of trematode migration may also be seen,10 as illustrated in the present case (Fig. 2). Given the protean manifestations and frequent overlap of pulmonary tuberculosis in areas of the world where paragonimiasis is common, tuberculosis is initially suspected CONCLUSIONS • In summary: • our patient presented with progressive cough and hemoptysis and was discovered to have a cavitary infiltrate on chest CT with a worm migration track. • Pathologic examination of lung tissue revealed ova diagnostic of pulmonary paragonimiasis likely contracted from eating undercooked, freshwater crustaceans in the patient’s native country of Burma. • Similar to many cases of paragonimiasis, the current case closely resembled pulmonary tuberculosis and emphasizes the need for a careful review of dietary habits and meticulous pathologic examination of tissue to ascertain the correct diagnosis. REFERENCES • Procop G. North American paragonimiasis (caused by Paragonimus kellicotti) in the context of global Paragonimiasis. ClinMicrobiol Rev. 2009;22:415-446. • Hu W. Studies on the life cycle of Paragonimus heterotremus.ZhongguoJi Sheng Chong Xue Yu Ji Sheng Chong Bing ZaZhi. 1998;16:347-352. • Diaz J. Boil before eating: paragonimiasis after eating raw crayfish in the Mississippi River Basin. J La State Med Soc. 2011;163:261-266. Figure 1: Computed tomography of the chest illustrating a large cavitary infiltrate in the right lower lobe.