Download
1 / 1
10 likes | 174 Views
OPTIONAL LOGO HERE. Referrals to Adolescent Gynaecology F Martyn, D Hayes-Ryan, O Sheil National Maternity Hospital, Holles St, Dublin. OPTIONAL LOGO HERE. Objectives. Methods.

E N D
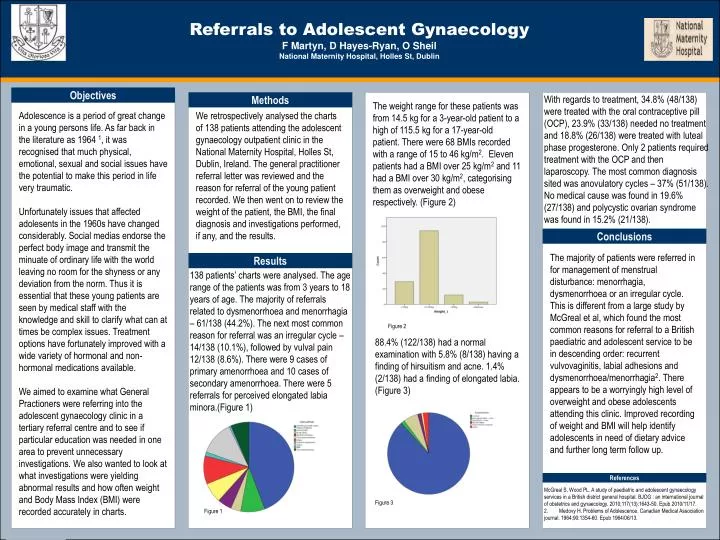
OPTIONALLOGO HERE Referrals to Adolescent Gynaecology F Martyn, D Hayes-Ryan, O SheilNational Maternity Hospital, Holles St, Dublin OPTIONALLOGO HERE Objectives Methods The weight range for these patients was from 14.5 kg for a 3-year-old patient to a high of 115.5 kg for a 17-year-old patient. There were 68 BMIs recorded with a range of 15 to 46 kg/m2. Eleven patients had a BMI over 25 kg/m2 and 11 had a BMI over 30 kg/m2, categorising them as overweight and obese respectively. (Figure 2) With regards to treatment, 34.8% (48/138) were treated with the oral contraceptive pill (OCP), 23.9% (33/138) needed no treatment and 18.8% (26/138) were treated with luteal phase progesterone. Only 2 patients required treatment with the OCP and then laparoscopy. The most common diagnosis sited was anovulatory cycles – 37% (51/138). No medical cause was found in 19.6% (27/138) and polycystic ovarian syndrome was found in 15.2% (21/138). Adolescence is a period of great change in a young persons life. As far back in the literature as 1964 1, it was recognised that much physical, emotional, sexual and social issues have the potential to make this period in life very traumatic. Unfortunately issues that affected adolesents in the 1960s have changed considerably. Social medias endorse the perfect body image and transmit the minuate of ordinary life with the world leaving no room for the shyness or any deviation from the norm. Thus it is essential that these young patients are seen by medical staff with the knowledge and skill to clarify what can at times be complex issues. Treatment options have fortunately improved with a wide variety of hormonal and non-hormonal medications available. We aimed to examine what General Practioners were referring into the adolescent gynaecology clinic in a tertiary referral centre and to see if particular education was needed in one area to prevent unnecessary investigations. We also wanted to look at what investigations were yielding abnormal results and how often weight and Body Mass Index (BMI) were recorded accurately in charts. We retrospectively analysed the charts of 138 patients attending the adolescent gynaecology outpatient clinic in the National Maternity Hospital, Holles St, Dublin, Ireland. The general practitioner referral letter was reviewed and the reason for referral of the young patient recorded. We then went on to review the weight of the patient, the BMI, the final diagnosis and investigations performed, if any, and the results. Conclusions The majority of patients were referred in for management of menstrual disturbance: menorrhagia, dysmenorrhoea or an irregular cycle. This is different from a large study by McGreal et al, which found the most common reasons for referral to a British paediatric and adolescent service to be in descending order: recurrent vulvovaginitis, labial adhesions and dysmenorrhoea/menorrhagia2. There appears to be a worryingly high level of overweight and obese adolescents attending this clinic. Improved recording of weight and BMI will help identify adolescents in need of dietary advice and further long term follow up. Results 138 patients’ charts were analysed. The age range of the patients was from 3 years to 18 years of age. The majority of referrals related to dysmenorrhoea and menorrhagia – 61/138 (44.2%). The next most common reason for referral was an irregular cycle – 14/138 (10.1%), followed by vulval pain 12/138 (8.6%). There were 9 cases of primary amenorrhoea and 10 cases of secondary amenorrhoea. There were 5 referrals for perceived elongated labia minora.(Figure 1) Figure 2 88.4% (122/138) had a normal examination with 5.8% (8/138) having a finding of hirsuitism and acne. 1.4% (2/138) had a finding of elongated labia. (Figure 3) References McGreal S, Wood PL. A study of paediatric and adolescent gynaecology services in a British district general hospital. BJOG : an international journal of obstetrics and gynaecology. 2010;117(13):1643-50. Epub 2010/11/17. 2. Medovy H. Problems of Adolescence. Canadian Medical Association journal. 1964;90:1354-60. Epub 1964/06/13. Figure 3 Figure 1