Download
1 / 36
360 likes | 474 Views
Medicare Update 2009. Roland A. Grieb, MD, MHSA Medical Director, Indiana Medicare Quality Improvement Organization January 14, 2009. Objectives. Understand the potential impact of value-based purchasing (VBP) on hospital health care

E N D
Medicare Update 2009 Roland A. Grieb, MD, MHSA Medical Director, Indiana Medicare Quality Improvement Organization January 14, 2009
Objectives Understand the potential impact of value-based purchasing (VBP) on hospital health care Define hospital-acquired conditions (HACs) and present on admission (POA) Recognize the key Recovery Audit Contractor (RAC) milestones, results, and lessons to date
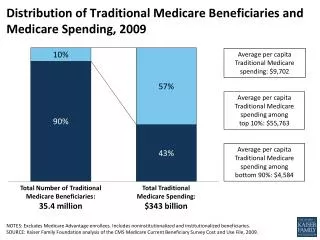
What Is Medicare Going to Do to Survive? Stefanacci, R., & Spivack, B. (2008). What is Medicare Going to Do to Survive? Annals of Long-Term Care , 16(12), 20-22. http://www.annalsoflongtermcare.com/content/what-is-medicare-going-do-survive • Three ways to make Medicare last longer and bring the costs down • Spread the costs of Medicare among Medicare beneficiaries • Reduce provider prices • Optimize utilization and benefits, and focus on quality of care
The Changing Face of Medicare Since Its Beginning Stefanacci, R., & Spivack, B. (2008). What is Medicare Going to Do to Survive? Annals of Long-Term Care , 16(12), 20-22. http://www.annalsoflongtermcare.com/content/what-is-medicare-going-do-survive
Medicare “R” Tools Stefanacci, R., & Spivack, B. (2008). What is Medicare Going to Do to Survive? Annals of Long-Term Care , 16(12), 20-22. http://www.annalsoflongtermcare.com/content/what-is-medicare-going-do-survive Reimbursement Regulations Resources Reporting
VBP and Hospitals • The Deficit Reduction Act (DRA) of 2005 mandated that the Centers for Medicare & Medicaid Services (CMS) develop a VBP program by FY 2009 • Also known as pay-for-performance (P4P) • Based on the purchasers using “market power” to drive quality improvement • No longer simply a “2% Gimme”
Report to Congress: Plan to Implement a Medicare Hospital VBP Program* • Options for implementing a VBP program in fiscal year (FY) 2009 presented to Congress in November 2007 * http://www.cms.hhs.gov/AcuteInpatientPPS/downloads/ HospitalVBPPlanRTCFINALSUBMITTED2007.pdf
Medicare Hospital Quality Improvement Act of 2008* • Senate Finance Committee Chairman Max Baucus and Ranking Member Charles Grassley released discussion draft of the Medicare Hospital Quality Improvement Act of 2008 on November 19, 2008 • Establishes Medicare VBP program for inpatient hospital care * http://finance.senate.gov/press/Bpress/2008press/prb111908c.pdf
Medicare Hospital Quality Improvement Act of 2008 (cont.) • Program would be built on the Medicare hospital pay-for-reporting program • Would link Medicare payments to how well hospitals actually perform on specific quality measures
Medicare Hospital Quality Improvement Act of 2008 (cont.) VBP program would initially measure performance in treatment of heart attacks, heart failure, pneumonia, and surgical care Would also measure overall patient satisfaction of hospital care Program would be initiated in FY 2012 and be fully implemented in FY 2016
Medicare Hospital Quality Improvement Act of 2008 (cont.) Payment levels would gradually increase from 1% in FY 2012 to 2% in FY 2016 Savings from reduced hospital payments would be kept in the hospital payment system in the form of increased payments to other hospitals
Medicare Hospital Quality Improvement Act of 2008 (cont.) • Addresses VBP demonstration program for inpatient critical access hospitals • The Secretary of Health and Human Services shall establish a demonstration program not later than two years after the date of enactment of this Act • Demonstration program shall be conducted for a three-year period
Medicare Hospital Quality Improvement Act of 2008 (cont.) • Not later than 18 months after completion of the demonstration program, the Secretary shall submit to Congress a report on the demonstration program • Include recommendations on the establishment of a permanent VBP program under the Medicare program for critical access hospitals with respect to inpatient critical access hospital services
Hospital-Acquired Conditions (HACs) • DRA Section 5001(c) is the statutory requirement for HACs conditions and POA • Translation • No increased payment for complicating conditions that are not present at the time of hospital admission • If the HAC is the only CC/MCC, then it will not lead to the higher paying DRG
Statutory Authority DRA Section 5001 (c) • Currently applies only to acute Medicare IPPS hospitals (those reimbursed under Diagnosis Related Groups [DRGs]) • Currently excludes critical access hospitals (CAH), psychiatric, and rehabilitation hospitals and distinct part units • Web source for HACs http://www.cms.hhs.gov/HospitalAcqCond/07_ EducationalResources.asp.
Hospital-Acquired Conditions (HACs) • CMS must select conditions that meet the following criteria • High-cost, high-volume, or both • Assigned to a higher paying DRG when present as a secondary diagnosis • “Reasonably preventable” through the application of evidence-based guidelines
CMS-Selected HACs • Foreign objects retained after surgery • Air embolism • Blood incompatibilities • Catheter-associated UTIs • Vascular catheter-associated infections • Pressure ulcers (Stages III & IV) Never Events Redefined
CMS-Selected HACs 7. Falls and other hospital-acquired injuries • Fracture, dislocation • Intracranial injury • Crushing injury • Burn • Electrical shock
CMS-Selected HACs New New • Manifestations of poor glycemic control • Hypoglycemic coma • Diabetic ketoacidosis • Nonketotic hyperosmolar coma • Secondary diabetes with ketoacidosis • Secondary diabetes with hyperosmolarity • Deep vein thrombosis (DVT)/pulmonary embolism (PE) • Total knee replacement • Hip replacement
CMS-Selected HACs New Additions New New • Surgical Site Infections • Mediastinitis after coronary artery bypass graft (CABG) • Certain orthopedic procedures • Spine • Neck • Shoulder • Elbow • Bariatric surgery for obesity • Laprascopic gastric bypass • Gastroenterostomy • Laparoscopic gastric restrictive surgery
What Does POA Really Mean? • Multiple clinical scenarios qualify as POA • Diagnosed prior to admission (e.g., history of diabetes) • Confirmed during the admission but documented at the time of admission as “suspected,” “possible,” “Rule/Out,” or as a differential diagnosis
What Does POA Really Mean? • Multiple clinical scenarios qualify as POA • Diagnosed after admission, but documented as an underlying cause of a symptom present at the time of admission • Present during an outpatient encounter prior to order for admission (e.g., ER, observation status, or outpatient surgery)
POA Reporting Options • Yes Present at the time of inpatient admission • No Not present at the time of inpatient admission • UInsufficient documentation to determine if condition is present on admission 4. W Clinically unable to determine whether condition was present on admission 5. 1 Exempt from POA reporting (unreported/not used)
Never Events in Indiana • Indiana State Department of Health (ISDH) Medical Errors Reporting Systems (MERS) Report • Hospital reportable events for 2007 • http://www.in.gov/isdh/23433.htm • Appendix B: hospital-specific data tables • Indiana hospitals and surgery centers committed 105 serious and preventable errors in 2007 • Approximately 24% increase from last year
RAC Program • Congress mandated the RAC program • Section 306 of the Medicare Modernization Act (MMA) directed the three-year RAC demonstration program • Section 302 of the Tax Relief and Healthcare Act (TRHCA) of 2006 required the RAC program become permanent and nationwide no later than January 1, 2010 • www.cms.hhs.gov/RAC
RAC Return on Investment (ROI) • Experienced a $4.60/$1 Benefit/Cost Ratio in FY 2007 • Benefit/Cost Ratio Calculation: $357.2M (total collections)/$77.7M (cost)= $4.60 • Spent only 22 cents for each dollar collected and returned to the Trust Fund • Cents Spent Per Dollar Saved Calculation: $77.7 M (cost)/$357.2M total collections = $.22 • Achieved a respectable ROI of 318% in FY 2007 • ROI Calculation: $357.2M (total collections) - $14.3 M (underpayments repaid) - $17.8 M (overturned on appeal) - $77.7 M (cost) = $247.4M (net savings)/$77.7 M (cost) = 3.18 * 100 = 318%
Transition to Permanent Program • October 2008: CMS announced names of permanent RACs for four regions • By 2010, CMS plans to have all four RACs in place • November 2008: Protest of RAC Awards and automatic stay • 100 days to issue decision • For further updates, go to www.cms.hhs.gov/RAC
Improvements to RAC Permanent Program • Look-back period reduced from four to three years • Will not be allowed to look at claims paid prior to October 1, 2007 (start of new Medicare Severity-DRG reporting) • Certified coders are required • CMS will set mandatory medical record limits • RAC Medical Director discussion
Improvements to RAC Permanent Program (cont.) • Required and frequent reporting of problem areas identified • Must pay back contingency fee if appeals are lost at any level • Must offer a Web-based application by January 1, 2010 • Uniform external RAC validation process is mandatory
Overview of Proposed RAC Process • Selection of claims for review • Must “target” claims through data analysis • Cannot randomly select claims • Cannot just focus on high payment claims
Overview of Proposed RAC Process • Types of RAC “targeted” reviews • Automated • No medical records involved in the review, certainty that overpayment exists based on data review • Complex • Medical records are involved in the review, high probability (but not certainty) that the service is not covered
Lessons Learned • Develop data mining tools • Purchase tools or develop on your own • Use data gleaned from knowledge of coding, DRGs, Program for Evaluating Payment Patterns Electronic Report (PEPPER) and Comprehensive Error Rate Testing (CERT) data, and RAC “mentality” • Internal Data Mining • High-Risk DRGs • High-Volume DRGs/High Volume Outpatient Services
Key Points • Realistically Indiana can anticipate the RAC for Region B to be in place by 2009 • Hospitals can avoid unnecessary denials by communicating directly with the RAC • RACs use same policies as Medicare Administrative Contractors (MACs) and QIOs Source: Medicare Recovery Audit Contractors: What are they, where are they? Melanie Combs, RN, RAC Technical Advisor Centers for Medicare & Medicaid Services (CMS) 35
QUESTIONS? Roland A. Grieb, MD, MHSA Health Care Excel (812) 234-1499, Extension 221 www.hce.org This material was prepared by Health Care Excel, the Medicare Quality Improvement Organization for Indiana, under contract with the Centers for Medicare & Medicaid Services (CMS), an agency of the U.S. Department of Health and Human Services. The contents presented do not necessarily reflect CMS policy. 9SOW-IN-GENE-09-001 01/13/2009