Download

1 / 34
400 likes | 828 Views
ABG’s. Blood gas slip. Data. Blood gases Electrolytes Haemoglobin Calculations Glucose “Balance”. What am I thinking ?. Importance of gases and acid base balance. Need oxygen to live Need to get rid of CO 2 a waste product Enzymes need pH 7.35 to 7.45 for optimal working.

E N D
Data • Blood gases • Electrolytes • Haemoglobin • Calculations • Glucose • “Balance”
Importance of gases and acid base balance • Need oxygen to live • Need to get rid of CO2 a waste product • Enzymes need pH 7.35 to 7.45 for optimal working
Gas exchange in the body Carbon dioxide Oxyygen Lungs Heart Body Tissues
Chemistry • C6H12O6 + 6O2 > 6CO2 + 6H2O • Glucose + Oxygen > Carbon dioxide + water • CO2 + H2O > H2CO3 > H+ + HCO3- • Carbon dioxide + water > carbonic acid > acid + bicarbonate • pH depends on H+
Energy use in the body Glucose Pyruvate TCA cycle Oxygen ATP Energy
Ways to loose acid • Lungs • Kidney
Glucose metabolism I Glucose Rest of body Muscle Liver Insulin
Glucose metabolism II • Glucose uptake depends on • Serum glucose • Blood flow • Insulin availability • Glucose doesn’t always cause acidosis
Lactic acid I Glucose No oxygen Lactic acid Pyruvate TCA cycle Oxygen ATP Energy
Lactic acid II - Lactic acidosis • Increased production • Tissue Hypoxia • Circulatory shock • Decreased utilisation • Liver failure • Circulatory shock • Acidosis dangerous, Lactate harmless • BE as surrogate marker
Calcium • Total calcium = free Ca2+ and Protein bound Ca2+ • Active form is free Ca2 • Myocardial contraction and vasoconstriction • NOT with radial artery • Calcium chloride and gluconate
Hct and haemoglobin • Bleeding • revealed • concealed • Chest • GIT • Retro peritoneum (IABP, recent angio)
Balance I • Most are 500mL to 2.0 L +Ve by am • Depend on • fluids/loses in theatre • pre op dehydration • An aid to diagnosing internal bleeding and excessive vasodilatation
Balance II • Always think (especially if CVP low) • Cold & 1.5L+Ve > CXR • Warm & 2.0 to 2.5L+Ve > CXR • Intra thoracic bleeding can occur regardless of chest tube drainage
Acid - Base balance • Metabolic “HCO3/other acid problem” • Produce / loose acid / alkali • Respiratory “CO2” problem • Produce / retain CO2
Base excess (BE)orHow much extra alkali • Meaning • Observation • Treatment
BE I - meaning • Normal ~ 0 • If –Ve acidosis of any cause is present • Circulatory insufficiency • Cardiac • Circulatory volume • Renal failure • Liver failure • Ischaemic limb eg IABP • Ischaemic bowel • Respiratory • If +Ve alkalosis • Chronic hypokalaemia
BE II - observation • A guide that patient is ok • If increasing negative monitor continuously • Can change from hour to hour
BE III - treatment • If BE < -6.0 to –8.0 negatively inotropic • Acknowledge there is a problem, give bicarb, monitor BE frequently to reassess
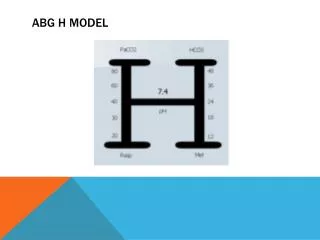
Blood gases I acid base balance • Uncompensated • No respiratory compensation when fully ventilated • Compensated • Most extreme value is usually primary problem • pO2 “unimportant” • CO2 + H2O > H2CO3 > H+ + HCO3- • Carbon dioxide + water > carbonic acid > acid + bicarbonate
Anion gap • What you can’t measure • (Na+ + K +) - (Cl - + HCO3 -) • Causes “KUSMAL” • Ketones • Uraemia • Salicylates • Methyl alcohol • Acid poisoning • Lactate
Frequency of blood gases? ½ Hr, 1 Hr, 2 Hr • Recent admission • Unstable • Bleeding • Oliguria/ renal failure • Liver failure • “just unwell” or “just not right” • Previously abnormal result • Change in ventilation • Good lungs 5 minutes poor lungs 20 to 25 minutes
ABG verses pulse oximetry • CO2 • Carbon monoxide
Calculated verses Measured oxygen • Different types of Haemoglobin • Oxyhaemoglobin • Reduced (Normal, but no oxygen bound) • Carboxyhaemoglobin (CO poisoning) • Methemoglobin • DPG, blood transfusions • Haemoglobinopathies