Download
1 / 1
10 likes | 248 Views
Summer Camp 2014. Please indicate which camp your teen will be attending: ( circle all you would like to attend) Session # 1: June 30 th – July 3 rd Session # 2: July 7 th – July 10 th Session # 3: July 14 th – July 17 th Session # 4: July 21 st – July 24 th

E N D
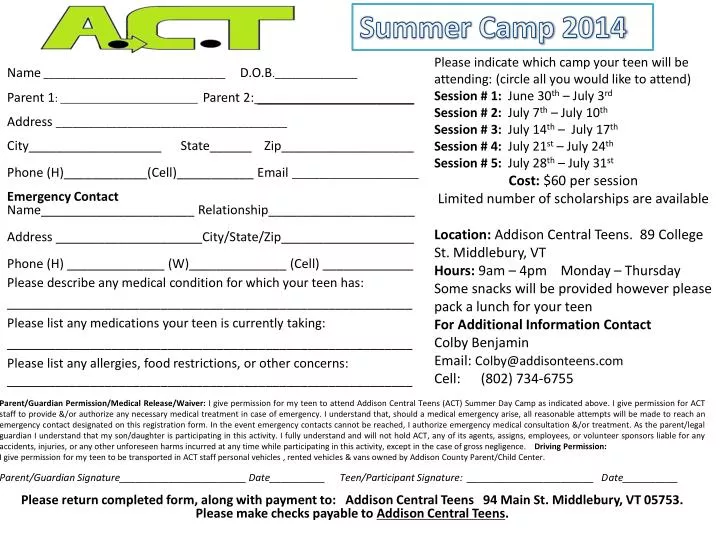
Summer Camp 2014 Please indicate which camp your teen will be attending: (circle all you would like to attend) Session # 1: June 30th – July 3rd Session # 2: July 7th – July 10th Session # 3: July 14th – July 17th Session # 4: July 21st – July 24th Session # 5: July 28th – July 31st Cost: $60per session Limited number of scholarships are available Location: Addison Central Teens. 89 College St. Middlebury, VT Hours: 9am – 4pm Monday – Thursday Some snacks will be provided however please pack a lunch for your teen For Additional Information Contact Colby Benjamin Email: Colby@addisonteens.com Cell: (802) 734-6755 Name _________________________________ D.O.B._______________ Parent 1: Parent 2:_____________________ Address __________________________________________ City___________________ State______ Zip___________________ Phone (H)____________(Cell)___________ Email _______________________ Emergency Contact Name______________________ Relationship_____________________ Address _____________________City/State/Zip___________________ Phone (H) ______________ (W)______________ (Cell) _____________ Please describe any medical condition for which your teen has: __________________________________________________________ Please list any medications your teen is currently taking: __________________________________________________________ Please list any allergies, food restrictions, or other concerns: __________________________________________________________ Parent/Guardian Permission/Medical Release/Waiver: I give permission for my teen to attend Addison Central Teens (ACT) Summer Day Camp as indicated above. I give permission for ACT staff to provide &/or authorize any necessary medical treatment in case of emergency. I understand that, should a medical emergency arise, all reasonable attempts will be made to reach an emergency contact designated on this registration form. In the event emergency contacts cannot be reached, I authorize emergency medical consultation &/or treatment. As the parent/legal guardian I understand that my son/daughter is participating in this activity. I fully understand and will not hold ACT, any of its agents, assigns, employees, or volunteer sponsorsliable for any accidents, injuries, or any other unforeseen harms incurred at any time while participating in this activity, except in the case of gross negligence. Driving Permission: I give permission for my teen to be transported in ACT staff personal vehicles , rented vehicles & vans owned by Addison County Parent/Child Center. Parent/Guardian Signature_______________________ Date__________ Teen/Participant Signature: _______________________ Date__________ Please return completed form, along with payment to: Addison Central Teens 94 Main St. Middlebury, VT 05753. Please make checks payable to Addison Central Teens.