Download
1 / 27
330 likes | 644 Views
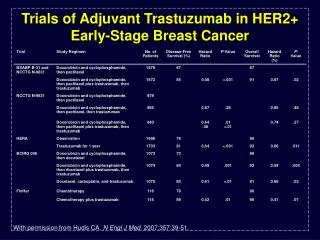
Adjuvant therapy of HER2 positive early breast cancer The Evidences. Antonio Frassoldati Oncologia Clinica - Ferrara. Evidences on adjuvant trastuzumab are based on randomized trials in over 14,000 women . S= sequential; C= concomitant

E N D
Adjuvant therapy of HER2 positive early breast cancerThe Evidences Antonio Frassoldati Oncologia Clinica - Ferrara
Evidences on adjuvant trastuzumab are based on randomized trials in over 14,000 women S= sequential; C= concomitant * Early release after second interim analysis (arm A, B) and first interim analysis (arm B,C)
Paclitaxel q3w x 4 AC q3w x 4 Paclitaxel x 4, H qw x 52 Carboplatin + Docetaxelq3w† x 6 H qw x 18, q3w x 12 Main trial designs of adjuvant Trastuzumab NSABP B-31 Node positive Paclitaxel qw x 12 N9831 Node pos/neg HR Paclitaxel qw x 12 H qw x 52 AC q3w x 4 Paclitaxel qw x 12, H qw x 52 BCIRG 006 Node pos/neg HR AC q3w x 4 Docetaxelq3w x 4 Docetaxelq3w x 4 AC q3w x 4 H qw x 12, q3w† x 14 HERA Chemotherapy (any) Node pos/neg HR Chemotherapy (any) H qw x 52 Chemotherapy (any) H qw x 104
Main research questions in trials of adjuvant trastuzumab • Does trastuzumab reduce the rate of recurrence (and death)? (All) • Does the schedule of trastuzumab administration matter? (N9831, BCIRG006) • Does the duration of trastuzumab matter? (HERA) • Does the chemotherapy regimen influence the activity and safety of trastuzumab? (BCIRG006)
Cross-comparison among the trials of adjuvant trastuzuamb ° Pts in HERA trial were randomized after the end of adjuvant therapy
B31/N9831Efficacy results Relapse HR 0.52 (0.45-0.60) Perez, JCO 2011
B31/N9831Efficacy results Death HR 0.61 (0.50-0.75) Perez, JCO 2011
HERA: DFS and overall survival over time Median follow-up (% follow-up time after selective crossover) Median follow-up (% follow-up time after selective crossover) No. of DFS eventsH 1 year vs. observation No. of deathsH 1 year vs. observation DFS benefit OS benefit 200511 year(0%) 200511 year (0%) 127 vs. 220p<0.0001 29 vs. 37p=0.26 200622 years(4.1%) 200622 years (4.3%) 59 vs. 90p=0.0115 218 vs. 321p<0.0001 200834 years (33.8%) 200834 years(30.9%) 182 vs. 213p=0.1087 369 vs. 458p<0.0001 0 1 2 0 1 2 Favourstrastuzumab Favours notrastuzumab Favourstrastuzumab Favours notrastuzumab HR HR 1. Piccart-Gebhart et al 2005; 2. Smith et al 2007; 3. Gianni et al 2011
HERA - Observation patients by status on 16 May 2005 1698 patients originally randomised to observation 1354 patients alive and disease free 344 patients DFS event or lost to follow-up198 alive post DFS event 2005 16 May 469 patients remained on observation 344 patients ineligible for crossover 885 patients crossed over to trastuzumab Gianni, Lancet Oncol 2011
HERA - DFS (landmark analysis): selective crossover and no crossover 100 80 60 Patients alive and disease free (%) 40 HR 0.68 (0.51-0.90) p=0.0077 20 Selective crossover*No crossover 0 0 6 12 18 24 30 36 42 48 Months from randomisation 885 885 884 878 870 851 822 690 480 No. at risk * Median time to start trastuzumab: 22.8 mos (4.5-52.7) Gianni, Lancet Oncol 2011 469 468 455 438 408 388 358 302 232
N9831Efficacy results Sequential vs Concomitant + sequential Perez, JCO 2011
BCIRG006Efficacy results DFS HR AC-TH vs AC-T 0.64 TCH vs AC-T 0.75 Slamon, NEJM 2011
FinHEREfficacy results Joensuu, JCO 2009
Efficacy of adjuvant trastuzuambon Survival ° ITT, not adjusted for selective crossover
Efficacy in subgroupsER and Nodal status AC-TH-H TCH Slamon, NEJM 2011
Time-dependent Hazard Rate for recurrence by hormone receptor status ER positive ER negative HERA trial Untch, Ann Oncol 2008
Efficacy in subgroupsSmall tumors 97.2% 86.4% MDACC Hazard Ratio for recurrence 5.3 965 pT1a-b N0 Gonzalez-Angulo, JCO 2009
Efficacy in subgroupsSmall tumors BCIRG006 Slamon, NEJM 2011
Efficacy in subgroupsTopo2A status With Topo2A coamplification Without Topo2A coamplification Slamon, NEJM 2011
Cardiac safety ° >10 points relative reduction in LVEF *after CT
HERA: risk-benefit ratio with adjuvant trastuzumaba Obs; DFS events H; DFS events H; any cardiac end point Obs; any cardiac end point 0.25 0.20 0.15 Probability 0.10 0.05 0.00 0 6 12 18 24 Monthsa No. at risk Observation 1693 1106 784 455 226 Trastuzumab 1139 861 520 260 1693 aMedian follow-up 12 months; DFS, disease-free survival Suter et al 2007
Cardiac outcomes after any type of cardiac endpoint Trastuzumab patients who have any type of CE (n=73) 19.2% 80.8% Trastuzumab patients who reached acute recovery after any type of CE (n=59) Trastuzumab patients who had a further LVEF drop to <50% (n=59) 28.8% 35.3% 71.2% 64.7%
Adjuvant HER2- directed Therapy Questions to be solved: • Indication for the better regimen for combination with trastuzumab (Anthracycline/taxane or docetaxel/carboplatin) • Role of shorter trastuzumab regimens • Treatment of triple-positive tumor migth avoid chemotherapy, particularly on small tumors (T1a,b N0) • Prediction of response to individual HER2-directed agents • Role of dual HER2 inhibition
Trastuzumab clearly changed the prognosis of HER2 breast cancer patients. Several new ways for further improvements can now to be explored HER2 street