Download
1 / 22
220 likes | 357 Views
PROGRAMA REGIONAL DE COOPERACIÓN CON MESOAMÉRICA “ Internship in Best Practices and Lessons Learned in Interagency Coordination Strategies for Overcoming Extreme Poverty". ANNA WILLIAMS, AG. DEPUTY DIRECTOR, HUMAN SERVICES DEPARTMENT

E N D
PROGRAMA REGIONAL DE COOPERACIÓN CON MESOAMÉRICA“Internship in Best Practices and Lessons Learned in Interagency Coordination Strategies for Overcoming Extreme Poverty" ANNA WILLIAMS, AG. DEPUTY DIRECTOR, HUMAN SERVICES DEPARTMENT DIANA POOK, CIVIC EDUCATION COORDINATOR, HUMAN SERVICES DEPARTMENT Ministry of Human Development, Social Transformation and PovertyAlleviation - BELIZE
Overview • National Poverty Elimination Strategy • Ministry of Human Development • Pro-poor programmes • Public Assistance • CCT: BOOST • Action and Results • Strengths and Weaknesses • Challenges • Expectations
Context I: Belize • Population Size: 0.3 Million • 80,000 HH • 31% Poor [2009, CPA] • HH which cannot meet basic food and non-food needs; poverty line: US$ 1,715.00 p.a. • 10% Extreme Poor [2009 CPA] • HH cannot meet basic food needs[cost of national food basket; indigent line: US$ 1,003.00 p.a
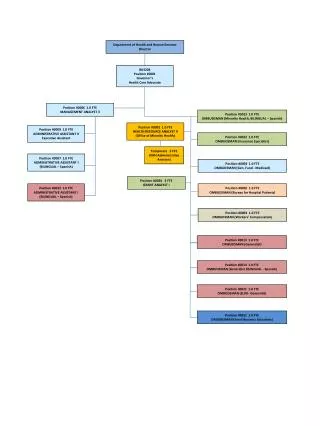
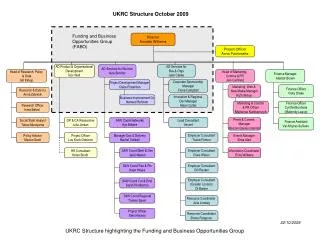
Institutional Arrangements Inter-Ministerial Social Sector Caucus [Social Cabinet]
MHDSTPA: Pro-Poor Programmes • Basic Social Services: Child Protection; Gender-base Violence • Public Assistance • Food • Rent • Medical • Education • Fire • Burial • Parenting and Early Childhood Stimulation • Subsidized Food Programme: Pantry • CCT Programme: BOOST
Context: “FromCountingthePoor” to “MakingthePoorCount” • Pre-2010: • Only able to quantify levels of poverty; • Rising and deepening levels of poverty • Counting the poor for > 3 decades • Interventions targeted at the district level • Post 2010: • BOOST Programme introduced • PMT endorsed by Cabinet • Identify and target poor and indigent HH • Shift from “counting the poor” to “making the poor count”
Building Opportunities for Our Social TransformationBOOST • CCT Scheme: differentiatedbenefitpaymentscheme • Education: 85% attendance • Health: • complete course of immunization • Early ante-natal visits [first 12 weeks] • Annualhealthchecksfortheelderly [60+] • Coverage: • 8300 beneficiaries in 3200 HH • 12.5% of poor HH; 6.1% of thepoor • 17% of extremelypoor HH [indigent] • 81% ‘bankarization’ rate
Benefit Payment • Elderly/persons with Disabilities: BZ$44.00/month • Children Age 0 – Std II: BZ$44.00/month • Std III – Form 4: Based on table below
Case Management • Case Management: • Families at risk of droppingout of thescheme • OVC [HIV and AIDS] • Supportservices: • birthregistration • Social securitycards
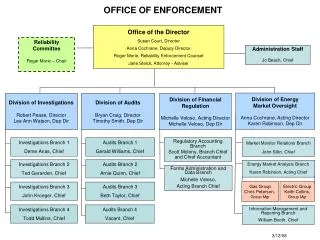
Intra-Ministerial Coordination • Programme is manage cross-unit • FSS: Programme Management • COMPAR: Compliance Monitoring • PPU: Targeting, MIS/M&E Support • Finance: Benefit payments/reconciliation
Inter-Ministerial Coordination • Ministry of Education • MOU • Compliance Monitoring: School Attendance • 286 Schools • Case Management Support • Beneficiaries dropped-out/at-risk of dropping out of school • Access to System Tools and use Common Protocols • BOWA; BOOST Handbooks
Inter-Ministerial Coordination • Ministry of Health • MOU: OVC Component of CCT Scheme • Access to system tools and complete HH intakes • HH Status Verification: affected/infected • Data exchange protocol • Basic excel password protected file • Compliance Verification: Immunization; early ante-natal care and health checks • Via BHIS [under development]
Strengths • National PRS exists and coordination entity identified • Achieved considerable gains in programme coverage and quality in short course • BOOST as a wider system leverage[reform]: • intra- ministerial: cross units and departments • inter-ministerial: MOH; MOE; MEDF • Fostering wider collaboration across SP agencies; early indications of convergence towards formalized social sector+ ministerial caucus[social cabinet] • Forging stronger programme linkages by design; integrated SSN with early discussions on “promotion” strategies • Contributing to a culture of M&E and evidence base practice • High degree of ‘goodwill’ among actors
Weaknesses • NHDAC collapsesunderitsownvolume and weight • Inadequatelyresourcedmechanisms • Lack of focus and follow-up • CommunicationIssues: inter-ministerial • Earlydays…leftto be seen
Challenges • Territorialism • Coordination in principle, progress is slow in practice • Paradigmshift: fromcountingthepoortomakingthepoorcount; counter-culture • Traditionally, lowadministrativecapacity in social service agencies nowrequiredtomanagecomplexprogrammes [CCT] • Shiftfromthe silo approachtoaneffective SSN requiringintegratedfamilyservices and intensive case management • Weak data systems and protocolsfor data sharing • ICT applications in SP: groundbreaking, limitedcapacities/experience
EXPECTATIVAS FRENTE AL TALLER • Explore opportunitiesforpolicylearning and transfer basedontheexperiences of countrieswithadvance/mature social servicesnetworks: