Download
1 / 129
1.31k likes | 1.63k Views
Covered by pages 1-49. Section 11. Radiation Therapy Clinical Treatment Management. Carl Bogardus, Jr, MD. 10:15 -10:45 AM. 031114. Modified For 04-11-14. 83. TOTAL CARE OF THE RADIATION ONCOLOGY PATIENT CLINICAL TREATMENT MANAGEMENT. 1.

E N D
Covered by pages 1-49 Section 11 Radiation Therapy Clinical Treatment Management Carl Bogardus, Jr, MD 10:15 -10:45 AM 031114 Modified For 04-11-14 83
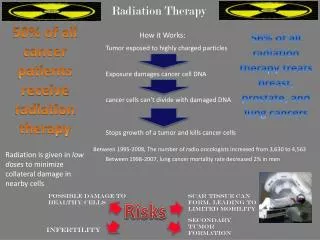
TOTAL CARE OF THERADIATION ONCOLOGY PATIENTCLINICAL TREATMENT MANAGEMENT 1 The total care of the radiation oncology patient mandates direct clinical management by the radiation oncologist throughout the course of therapy. It is the radiation oncologist’s role and responsibility to provide daily supervision of treatment and hands-on, face-to-face patient care.
Clinical Treatment Management Clinical Treatment Management starts with the acceptance of the patient for treatment. Clinical Treatment Management ends with the Clinical End of Treatment report. Clinical Treatment Management is tied to 5 days of treatment delivery only as a convenient means of tracking time for billing purposes. 2
CPT Radiation Therapy Treatment Management Codes 4 77427 -Weekly Radiation Therapy Management, 5 fractions 77431 -Radiation Therapy Management; Short course, 1 or 2 fractions 77432 -Radiation Therapy Management; Stereotactic, (SRS) 1 fraction 77435 –Radiation Therapy Management; SBRT, SRS, full course of therapy, up to a max of 5 fractions, (2007) 77469- Radiation Therapy Management; Intraoperative.
4 Professional billing 77427 • Professional billing relates to 5 fractions of therapy delivered, regardless of the number of elapsed calendar days and must be billed as 77427 X 1 per 5 FX block of treatments. • The billing date for weekly management , 77427, is usually the first day of each of the 5 day blocks.
NIB Most of the Carriers want you to report this way 5 fractions equal one Week, bill first date of week
Historical Background 7 • It is imperative that each physician document their direct involvement in all of the procedures related to a week of treatment management. • It is expected that each patient will have as many regularly spaced progress notes as there are weeks of treatments. • The complexity and completeness of the note must reflect the complexity of care for the patient.
7 WEEKLY UNDER BEAM PROGRESS NOTES Five Required Review Elements The physician will be expected to have reviewed as many of these elements as are applicable to the current course of treatment management It is extremely important that these five critical elements be covered in each note. I Chart and dosimetry review II Treatment setup and delivery review III Port film or electronic image review IV Under beam evaluation of the patient V Recommendation of therapy
8 • The weekly progress note does not necessarily have to occur on the same day of each week, but for a course of therapy there should be an equal or greater number of progress notes than the weeks of management being billed.
9 Mon Tues Wed Thurs Fri Week TX TX TX TX TX 1 NO PROGRESS NOTE WEEK 1 This causes problems with 77427 Week TX TX TX TX TX 2 PN 77427 Week TX TX TX TX TX 3 PN 77427 Week TX TX TX TX TX 4 PN 77427 A weekly note must occur sometime during each 5 day interval
9 Mon Tues Wed Thurs Fri Week TX TX TX TX TX 1 PN Having a note on week 1 is crucial 77427 Week TX TX TX TX TX 2 PN 77427 Week TX TX TX TX TX 3 PN 77427 Week TX TX TX TX TX 4 PN 77427 Having a note on the last TX date is very important PN 77427 EOT A weekly note must occur sometime during each 5 day interval
9 WEEKLY PROGRESS NOTE • There is no written directive stating which day during the treatment week that the physician/patient encounter must occur. • There is no stipulation of the manner of interaction, only that it be “face to face”
9 Parking garage Hall way Waiting room Exam room Treatment console Treatment room Which is a valid location for patient/physician encounter?
10 ALL OF THEM • At each encounter this patient had the opportunity ask question related to her course of treatment. • At each encounter the patient acknowledges her interaction with the physician. • At each encounter the physician has the opportunity to evaluate the patient’s general condition. • At each encounter the physician will use his best judgment to determine what is needed to evaluate response to treatment and radiation reactions • There is no written requirement related to length of time or location of the patient/physician encounter • As long as privacy concerns are met to the satisfaction of both the physician and the patient. 20/104
10 WEEKLY PROGRESS NOTE • The patient /physician encounter is only one of the 5 required elements of weekly management • The weekly progress note is a document covering all aspects of patient care and management. • Each of the 5 basic elements is further subdivided into many sub routines that require individual documentation
10 WEEKLY PROGRESS NOTE • The production of this supporting document does not need to coincide with the physical examination of the patient. • It is customary done this way only as a general convenience, not a requirement
NIB Narrative on page 6 INITIAL EVALUATION DOSIMETRY TREATMENT IMAGING EXAMINATION UNDER BEAM PROGRESS NOTES CLINICAL END OF TREATMENT SUMMARY The under beam progress note is a clinical weekly summary documentingthe physician’s involvement in the weekly management of the patient FOLLOW UP NOTES Using the cascading Information format, vital clinical and technical data may be transferred, discarded, or added to each new weekly document as it is created
Compliance and audits. These are two words that most physicians and administrators really don't like to hear. With cascading, elements of an E/M document will copy verbatim into subsequent documents. Verbatim copying will cause cascading of old information into new encounter forms without any change. Medicare considers that an identically copied note indicates that the physician was not actively involved in the creation of the new note. Templating has HCFA considering severe penalties when they find large sections of notes that are 100% copies in subsequent workups. NIB
NIB All physicians and users should be very much aware of this potential problem. They are well advised to carefully read any areas of their notes that are likely to change such as; Chief Complaint, HPI, Physical Exam Review of Systems Medical decision-making Other areas may also change. Do not always use exactly the same time for every patient or type of encounter.
NIB Compliance Warning, Cascaded Information
NIB Original work up Six week follow-up
All that is really required is a quick review of the areas of a document where you know some changes have probably occurred based upon the patient's clinical findings and treatment parameters. Document those changes in the record. If no changes have occurred, indicate that you have reviewed that section and it is truly unchanged from the previous work up. EMRs make compliance very easy, but they also make auditing very easy. NIB
We Recommend NIB • Any cascaded topic that has not been reviewed on a new document will clear upon save and record. • If the topic has been opened and any change has been made, then the changed topic and its questions and answers will be saved. • You may indicate “reviewed and save, no change needed”.
# 1--Chart & Dosimetry Review 15 • Verification of correctsummation of dose • Verify thattime and/or monitor unitsare correct. • Stop or re-evaluation pointsare clearly indicated. • The correctmodalities of treatment are indicated. • The correct beam energy is indicated. • Proper beammodifiersare in place. • Tumor dose is compared to thetolerance doseofcritical tissues. • Critical tissuedose pointsare carried • The number oftreatment volumesis correct. • The numberof ports is correct. Document of the first day of treatment with the first under beam note
15 #2 Treatment Setup & Positioning Evaluation It is understood that it is impossible for the physician to be physically present during each and every setup, butthe physician should be readily available for corrective action should the need arise. Document of the first day of treatment with the first under beam note
16 # 3--Portal Film Review for Imaging Radiographic films or electronic or portal imaging studies are taken at regular intervals of all of the portals being treated. Port film review must be documented each week in the under beam progress note, if imaging is performed.
16 # 4--UNDER BEAM EVALUATION PROGRESS NOTE Examination of the patient consists of clinical evaluation, assessment of tumor response, and case management. The radiation oncologist should physically examine the patient each week for treatment related side effects, and tumor response.
17 Under Beam Examination - Every patient under treatment, without exception, should be seen and examined at least once per week by the physician. This is a key element of the weekly note. The PA can do much of the work, but the physician must be involved
17 For under beam visits, these components are the same as for other E/M services. E/M services are included in weekly management and cannot be charged separate. 44/104
17 Many factors make up a weekly progress note, the use of multiple choice questions with many choices of answers, makes each note unique and reduces the appearance of “macro copying”
NIB Pages 17 to 20 give a short summary of the needed elements to make up a compliant progress note. You should follow these guide lines to format the content of your notes.
21 UNDER BEAM PROGRESS NOTE Every progress note should have the basic demographic information about the patient.
21 History of Present Illness A very short version of the patient's present illness should be presented limited to only a few sentences summarizing the case to-date.
22 Current Treatment Parameters Area(s) under treatment Energy/mode Evaluation of appropriateness and accuracy of all Treatment Devices Current dosage Planned dosage Critical structure dosage Microdosimetry as done Any corrective action as required
A weekly review of technical factors is required, once entered, this component usually will not vary week to week, if any factors change, then the note must reflect the changes 22
23 Physical Examination Constitutional General appearance Examination of area under treatment must always be included Examination of other areas as needed
24 Current Status of any Treatment Reactions Skin reactions GI reactions Oral cavity reactions Hematologic profile Present weight as related to previous weight
24 Tumor Response Indicate any changes from previous work-up Significant or subtle changes in tumor size Expected response at current dose level
Pain Assessmentand Management See Section 3 Page 8 • Full assessment of pain • Medications and corrective actions • Order and document medications • Print prescriptions • Maintain a compliant list of all medications and prescriptions. ONCOCHART
25 #5 Recommendation of Treatment • Patient to continuetherapy • Patient placed on hold – state the reason • Treatment requires modification • Patient has completed the course of treatment • THIS MUST BE COMPLETED BY THE PHYSICIAN EACH WEEK, NO OTHER PERSON CAN MAKE THIS DECISION.
Physician orders (CPO) 25 • With electronic records, Clinical Physician Orders have been made much easier to deal with. • Multiple paper forms are eliminated • Orders can be tailored to fit the case • Orders can be sent electronically
25 Physician work page has all the common procedures that require orders. This can be initiated by any authorized person in the department A narrative is produced which can be sent electronically, faxed, or printed THIS IS A MEANINGFUL USE REQUIREMENT ONCOCHART
Drug Orders in Dept. Electronic record of physician order for medication dispensed by nursing staff and signed off by physician. Compliant with JCAHO and Meaningful Use.
26 Clinical comment regarding Current Status • This is a brief narrative summary of a review of any of the preceding elements that show significant change, or new developments of importance to the care of the patient. ONCOCHART
Coordination of Care 26 • Routine progress notes should be sent to the patient’s other physicians to keep them informed of the case under treatment. 60/104
26 Physician Demographics • Every progress note should conclude with a signature of the physician of record and indication of copies to other physicians or charts. • Electronic signature is acceptable if original signature is on file.
27 Check-off and fill-in weekly summaries are marginally acceptable, but they must be legible and complete. They must show that the physician has documented his/her direct involvement in the production of the weekly assessment.
NIB THIS NOTE DOES NOT MEET MEANINGFUL USE, WHICH IS NOW REQUIRED This check off note just barely will suffice as a valid progress note. Demographics, vitals, dose, and some recommendation of therapy are noted, but the rest is almost unintelligible, and far too brief, with many key elements missing, such as a legible signature and physician name.
NIB This weekly under beam note is also marginal in terms of useful data, and does not meet compliance requirements.
NIB NIB Electronically Generated Progress Notes are Preferable