Download
1 / 16
180 likes | 392 Views
Simulation teaching on Depression at the University of Zimbabwe. Dr. Chido Rwafa. Background. ‘IMHERZ’(Improving Mental Health and Research in Zimbabwe) launched in 2009 as part of MEPI (Medical Education Partnerships Initiative) program.

E N D
Simulation teaching on Depression at the University of Zimbabwe Dr. Chido Rwafa
Background • ‘IMHERZ’(Improving Mental Health and Research in Zimbabwe) launched in 2009 as part of MEPI (Medical Education Partnerships Initiative) program. • Aims are to increase and retain mental health specialists in Zimbabwe. • Aim to revise undergraduate curriculum and introduce novel teaching methods as part of IMHERZ’s work.
Background • No available literature on simulation teaching in Psychiatry in Africa. • Studies from UK show that interactive learning through case-based discussions and role-play is superior to didactic lectures (Simmons and Wilkinson 2012). • US literature suggests use of simulation to counteract inconsistencies in clinical teaching (IssenbergMcGaghie et al 2005). • Simulation: ‘clinical scenarios whereby the patient is played by someone coached to show signs and symptoms of a real patient.
Background • Current undergraduate Psychiatry curriculum is delivered by didactic lectures, clinical attachment and case presentations once weekly. • Challenges of small number of faculty to provide undergraduate and postgraduate teaching as well as clinical duties. • Attachments take place on psychiatric inpatient wards and outpatient clinics, limited exposure to common mental disorders.
Objectives • To introduce a simulation teaching session into the Depression module on the undergraduate psychiatry program. • To conduct an evaluation of teaching to assess the impact of this intervention on students’ clinical skills compared to a hand-out on Depression. • To assess effectiveness of simulation teaching in terms of building confidence and student enjoyment.
Methods • Pre-pilot work in 2011: 10 students took part in voluntary simulation sessions and provided positive feedback. • January 2013, 30 4th year medical students randomly divided into 2 groups, half received simulation teaching in week 2 (group 1), half received session in week 6 (group 2). • Group 2 received MhGAP hand-out on management of Depression prior to OSCEs. • OSCEs took place week 4: results for groups 1 and 2 compared.
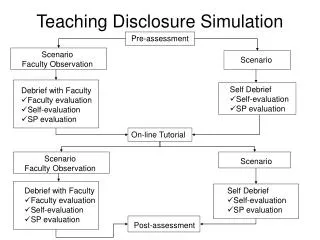
Simulation sessions • Short didactic 20 minutes focussed on history taking in Depression and communication skills. • Nursing staff recruited and trained to be simulated patients (SPs). • 3 clinical scenarios; students divided into small groups (N= 4-5) and rotate around 3 scenarios. • At each scenario, one student interviews SP. Peers, SP and facilitator provide feedback.
OSCEs • Each student undertakes 3 clinical scenarios on Depression- 2 history-taking, 1 explanation. • Session with faculty beforehand to adapt mark-sheet. • Scored by examiner and SP.
Preliminary Results • All students reported increased confidence in assessing and managing a patient with Depression following the simulation session. • Free text feedback was positive overall.
Preliminary Results • Overall scores: Simulation group- 69.94% Non-simulation group- 72.84% • Students in day 2 of OSCEs did better overall: Day 1 average: 63.86% Day 2 average: 72.63% • On day 1, students who had received simulation session did better (ave score 7.5% better). S group (n=9): 66.43% Non S group (n=5): 59.05% • On day 2, students who had received the simulation actually did worse S group (n=4): 66.35% Non S group (n=9): 75.19%
Discussion • This was a pilot study to pilot the use of simulation teaching and assessment with OSCEs • The students found it useful and free text feedback was generally positive • Students tended to get similar scores across 3 stations- suggests good inter-station reliability of stations.
Discussion • No Statistical significance between the simulated and non simulated groups (69.94% and 72.84% with 15 students in each group) • However the day 2 results were generally higher than the day 1 results, this may have been due to: Students coaching each other? Examiners more lenient? Simulated patients more generous? Small numbers= Insufficient power
Lessons learned • Experience of simulation teaching positive overall and it did not make things worse • Simulation teaching now implemented as standard in 4th year Psychiatry curriculum. • Experience of OSCEs; need for communication skills in clinical years? • OSCEs not yet established as summative assessment in Psychiatry, may be introduced in future.
Lessons Learned • A future study…with larger numbers to demonstrate statistical significance • Factors to consider in a future study… • MMeds involved in delivering simulation teaching- sustainability and support for faculty. • Further recruitment and training of simulated patients required- some problems with using nurses.