Download
1 / 1
130 likes | 1.15k Views
ABDOMINAL PREGNANCY Faisol Mihat, Dharma N., Eliza M. Noor, Ravichandran J. Hospital Sultanah Aminah, Johor Bahru, Malaysia. OPTIONAL LOGO HERE. OPTIONAL LOGO HERE. Objectives. Case Report. Case Report. Conclusions.

E N D
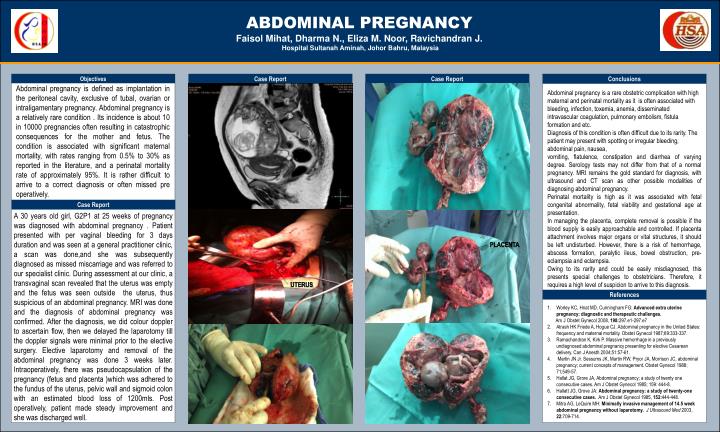
ABDOMINAL PREGNANCY Faisol Mihat, Dharma N., Eliza M. Noor, Ravichandran J. Hospital Sultanah Aminah, Johor Bahru, Malaysia OPTIONALLOGO HERE OPTIONALLOGO HERE Objectives Case Report Case Report Conclusions Abdominal pregnancy is defined as implantation in the peritoneal cavity, exclusive of tubal, ovarian or intraligamentary pregnancy. Abdominal pregnancy is a relatively rare condition . Its incidence is about 10 in 10000 pregnancies often resulting in catastrophic consequences for the mother and fetus. The condition is associated with significant maternal mortality, with rates ranging from 0.5% to 30% as reported in the literature, and a perinatal mortality rate of approximately 95%. It is rather difficult to arrive to a correct diagnosis or often missed pre operatively. Abdominal pregnancy is a rare obstetric complication with high maternal and perinatal mortality as it is often associated with bleeding, infection, toxemia, anemia, disseminated intravascular coagulation, pulmonary embolism, fistula formation and etc. Diagnosis of this condition is often difficult due to its rarity. The patient may present with spotting or irregular bleeding, abdominal pain, nausea, vomiting, flatulence, constipation and diarrhea of varying degree. Serology tests may not differ from that of a normal pregnancy. MRI remains the gold standard for diagnosis, with ultrasound and CT scan as other possible modalities of diagnosing abdominal pregnancy. Perinatal mortality is high as it was associated with fetal congenital abnormality, fetal viability and gestational age at presentation. In managing the placenta, complete removal is possible if the blood supply is easily approachable and controlled. If placenta attachment involves major organs or vital structures, it should be left undisturbed. However, there is a risk of hemorrhage, abscess formation, paralytic ileus, bowel obstruction, pre-eclampsia and eclampsia. Owing to its rarity and could be easily misdiagnosed, this presents special challenges to obstetricians. Therefore, it requires a high level of suspicion to arrive to this diagnosis. Case Report A 30 years old girl, G2P1 at 25 weeks of pregnancy was diagnosed with abdominal pregnancy . Patient presented with per vaginal bleeding for 3 days duration and was seen at a general practitioner clinic, a scan was done,and she was subsequently diagnosed as missed miscarriage and was referred to our specialist clinic. During assessment at our clinic, a transvaginal scan revealed that the uterus was empty and the fetus was seen outside the uterus, thus suspicious of an abdominal pregnancy. MRI was done and the diagnosis of abdominal pregnancy was confirmed. After the diagnosis, we did colour doppler to ascertain flow, then we delayed the laparotomy till the doppler signals were minimal prior to the elective surgery. Elective laparotomy and removal of the abdominal pregnancy was done 3 weeks later. Intraoperatively, there was pseudocapsulation of the pregnancy (fetus and placenta )which was adhered to the fundus of the uterus, pelvic wall and sigmoid colon with an estimated blood loss of 1200mls. Post operatively, patient made steady improvement and she was discharged well. placenta uterus References Worley KC, Hnat MD, Cunningham FG: Advanced extra uterine pregnancy: diagnostic and therapeutic challenges. Am J Obstet Gynecol 2008, 198:297.e1-297.e7 Atrash HK Friede A, Hogue CJ. Abdominal pregnancy in the United States: frequency and maternal mortality. Obstet Gynecol 1987;69:333-337. Ramachandran K, Kirk P. Massive hemorrhage in a previously undiagnosed abdominal pregnancy presenting for elective Cesarean delivery. Can J Anesth 2004;51:57-61. Martin JN Jr. Sessums JK, Martin RW, Pryor JA, Morrison JC, abdominal pregnancy; current concepts of management. Obstet Gynecol 1988; 71;549-57. Hallat JG, Grore JA, Abdominal pregnancy; a study of twenty one consecutive cases. Am J Obstet Gynecol 1985; 159: 444-8. Hallatt JG, Grove JA: Abdominal pregnancy: a study of twenty-one consecutive cases. Am J Obstet Gynecol 1985, 152:444-448. Mitra AG, LeQuire MH: Minimally invasive management of 14.5 week abdominal pregnancy without laparotomy. J Ultrasound Med 2003, 22:709-714.