Download
1 / 24
250 likes | 449 Views
Selection and Payment of Health Care Providers. Flagship Course on Health System Strengthening in Africa Kigali, June 24 th , 2010 Driss Zine-Eddine El- Idriss , HSO Hub/World Bank [Special thanks to HS20-20]. Objectives. Understand and apprehend:

E N D
Selection and Payment of Health Care Providers Flagship Course on Health System Strengthening in Africa Kigali, June 24th, 2010 DrissZine-Eddine El-Idriss, HSO Hub/World Bank [Special thanks to HS20-20]
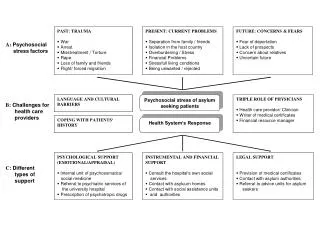
Objectives Understand and apprehend: • goals of schemes in selecting and paying providers; • how to lay the groundwork for selecting and engaging health care providers; • key factors in the design of rational payment systems; • key aspects to strengthening service delivery to assure good quality and efficient health care provision.
Some preliminary questions Questions for Health Insurers as purchasers: • For whom should I buy health services? [Population coverage; Targeted groups] • What should/could I buy? [Benefits package] • From whom should I buy? [Selection of Health Providers] • How should I buy? [Contracting & Providers Payment Mechanisms]
Purchasing • Passive purchasing • No selectivity of providers • No quality control and monitoring • Use of norms to set fees and related concerns • Strategic purchasing • Performance-based model • Contestable contracts • Ongoing quality control and monitoring ...
Incentives: the heart of the system Purchaser (insurer) Incentives Beneficiaries Providers
Aligning Goals with Selection and Payment of Providers • Payment systems create incentives for providers and patients/beneficiaries • Align health insurance policy goals with choices of providers and payment methods • Policy goals may include: Access, quality, cost containment, equity, preventive vs curative care, simplicity, prevention of fraudulent behavior etc.
Understand the Offer/Supply • Understand the supply of health care providers • Provider type, number and location relative to target population and benefits package • Health insurance schemes require adequate provider networks • HI schemes can promote but usually cannot create the desired mix and numbers of providers • Map providers to service areas
Understand the Offer/Supply Compare mapping to goals, benefits, target populations • Make adjustments as necessary • Either in goals, benefits, target populations or in pre-requisites to implementing scheme to create adequate network • Bonus: mapping helps in your negotiations with insurance companies etc., to ensure they contract with adequate provider network
Choice of Providers • Choice of providers is often important to beneficiaries • Must be balanced with healthinsurance goals and realities • Types of choices: • Public vs. private • Choice among similar specialties • Generalists vs. specialists (gatekeepers?) • Physicians Vs. other health care workers • Types of hospitals (clinics, secondary, tertiary, ER) • In network vs. out-of-network (often not option in developing countries)
Choice of Providers • Impacts (tradeoffs) of decisions on provider choice • Beneficiary satisfaction • Cost and efficiency • Provider income • Quality/appropriateness of care
Quality of Care Provider contracting and payments are not primary determinants of quality but can have a significant impact • Cross element point: Health insurance is not a panacea for what ails a health care system • But can help to address some system issues such as access, quality, equity…
Payment & contracting can affect quality • Ways that selection, contracting and payment can affect quality: • Require accreditation and/or Quality Assurance • Align physician and hospital incentives with appropriate care • Balance of PHC and specialist professionals in network • Beneficiary complaint resolution process • Financial incentive for appropriate number, type and location of care • Compliance with clinical guidelines • Example; Clinical care pathways (CCP) for hospital payments • Require participation in quality assurance program • Termination from network and other penalties
Provider Payment Modalities • Typology: • Fee-for-service • Capitation • Line item budgets • Per-diem • Case-based payments • Global budget • Performance-based payments (P4P) • Many variations on each (and this list is not exhaustive) • Can get extremely complex • Politics and influence will always play a part
Provider Payment Modalities • Fee-for-service • Payment is made for each service provided • Many variations on FFS payment methodology • Capitation • Fix amount per member (or sometime group) per month/year for specified basket of services • Most common for PHC
Provider Payment Modalities • Line-item budget (hospitals and clinics) • Based on inputs (number of beds, physicians, health workers, buildings etc.), rather than outputs (e.g., services provided) • Common in former socialist countries and public facilities • Can be adjusted to take some measures of output into account • Per-diem (hospitals) • Fix payment for each day patient is in hospital (per bed-day) • Can be case-mix adjusted and have limits by diagnosis
Provider Payment Modalities • Case-based payment (hospitals) • Fixed payment for a case based on diagnosis (or variation) • Many types have been developed (e.g. diagnostic-related groups), • Adjustments for outliers, hospital case-mix • Complex to implement • Data requirements, coding, training, groupers, upcoding
Provider Payment Modalities • Global Budget • Fixed maximum expenditure for basket of services • Can be based on factors such as: Health care needs; objective target (e.g., % GDP) etc. • Budgets usually set by governments (e.g. Canada single payer, German point system) • Enforcement is an issue • Performance-based payments (P4P or value-based purchasing) • Links payments to pre-determined result or output • Can link to positive results or decreasing negative results (e.g., medical errors) • Questions from providers on appropriateness of quality measures
PPM Features Adapted from: PHR (1998)
Operational & Institutional Constraints • Provider selection systems can range from simple to very complex • More complex strategies have tried to align various policy goals and incentives • Need to carefully consider • Data and information available to support various payment methods • Regulations and requirements (e.g., use of ICD-10 codes) • Information technology available: groupers, HMIS; Automation available at hospitals, clinics group practices • Human resource capacity • Training requirements
Requirements Source: PHR
Provider Contracts • Provider contracts must: • Conform to legal and regulatory requirements of the jurisdiction • Cover essential elements clearly: • Covered services • Payment rate and terms • Dispute resolution • Performance incentives; • Indemnification and liabilities • Administrative procedures (forms, billings) • Both parties’ rights
Payment modalities & Providers’ behavior Effect: +++ very positive; ++ some positive; +/- little or variable; -- some negative; --- very negative Source: WHO
Optional Exercise • How do insurers determine the adequacy of the providers’ network in your country? • What kinds of PPM are used in your country? • What are incentives in each PPM? • Is it easy to move from one PPM to another? • Is it relevant to combine multiple PPM?