Download
1 / 1
10 likes | 246 Views
. Successful full term pregnancy in a woman with Didelphys uterus.- Case report. Dr.Purnima.Deb.DGO.MD. FRCOG. FICOG -Consultant Al Wasl hospital , Dubai. Dr.Abeer Gergawi.ABOG.Specialist registrar –Al Wasl hospital Dubai. Dr.Laila Al Hubaishi- Senior house officer,Al Wasl hospital,dubai.

E N D
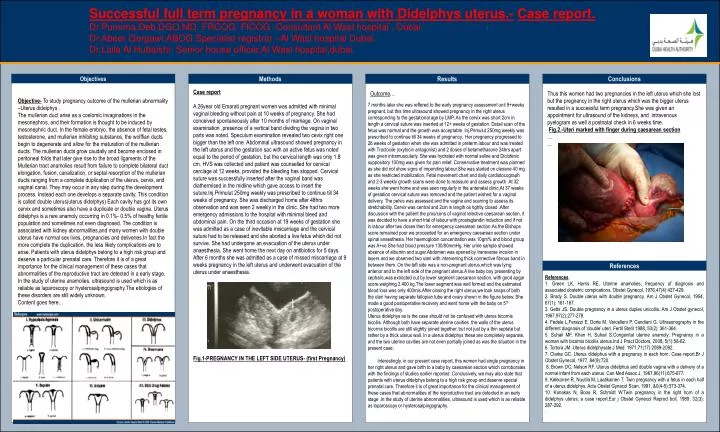
. Successful full term pregnancy in a woman with Didelphys uterus.-Case report. Dr.Purnima.Deb.DGO.MD. FRCOG. FICOG -Consultant Al Wasl hospital , Dubai. Dr.Abeer Gergawi.ABOG.Specialist registrar –Al Wasl hospital Dubai. Dr.Laila Al Hubaishi- Senior house officer,Al Wasl hospital,dubai. OPTIONALLOGO HERE . . . . Objectives Methods Results Conclusions Case report A 26year old Emarati pregnant women was admitted with minimal vaginal bleeding without pain at 10 weeks of pregnancy. She had conceived spontaneously after 10 months of marriage. On vaginal examination ,presence of a vertical band dividing the vagina in two parts was noted. Speculum examination revealed two cevix right one bigger than the left one. Abdominal ultrasound showed pregnancy in the left uterus and the gestation sac with an active fetus was noted equal to the period of gestation, but the cervical length was only 1.8 cm. HVS was collected and patient was counselled for cervical cerclage at 12 weeks, provided the bleeding has stopped. Cervical suture was successfully inserted after the vaginal band was diathermised in the midline which gave access to insert the suture.Inj.Primulut 250mg weekly was prescribed to continue till 34 weeks of pregnancy. She was discharged home after 48hrs observation and was seen 2 weekly in the clinic. She had two more emergency admissions to the hospital with minimal bleed and abdominal pain. On the third occasion at 19 weeks of gestation she was admitted as a case of inevitable miscarriage and the cervical suture had to be released and she aborted a live fetus which did not survive. She had undergone an evacuation of the uterus under anaesthesia. She went home the next day on antibiotics for 5 days. After 6 months she was admitted as a case of missed miscarriage at 9 weeks pregnancy in the left uterus and underwent evacuation of the uterus under anaesthesia. Fig.1-PREGNANCY IN THE LEFT SIDE UTERUS- (first Pregnancy) Objective-To study pregnancy outcome of the mullerian abnormality –Uterus didelphys . The mullerian duct arise as a coelomic invaginations in the mesonephros, and their formation is thought to be induced by mesonephric duct. In the female embryo, the absence of fetal testes, testosterone, and mullerian inhibiting substance, the wolffian ducts begin to degenerate and allow for the maturation of the mullerian ducts. The mullerian ducts grow caudally and become enclosed in peritoneal folds that later give rise to the broad ligaments of the Mullerian tract anamolies result from failure to complete bilateral duct elongation, fusion, canalization, or septal resorption of the mullerian ducts ranging from a complete duplication of the uterus, cervix, and vaginal canal. They may occur in any step during the development process. Instead each one develops a separate cavity. This condition is called double uterus(uterus didelphys) Each cavity has got its own cervix and sometimes also have a duplicate or double vagina. Uterus didelphys is a rare anamoly occurring in 0.1%- 0.5% of healthy fertile population and sometimes not even diagnosed. The condition is associated with kidney abnormalities,and many women with double uterus have normal sex lives, pregnancies and deliveries.In fact the more complete the duplication, the less likely complications are to arise. Patients with uterus didelphys belong to a high risk group and deserve a particular prenatal care. Therefore it is of a great importance for the clinical management of these cases that abnormalities of the reproductive tract are detected in a early stage. In the study of uterine anamolies, ultrasound is used which is as reliable as laparoscopy or hysterosalpingography.The etiologies of these disorders are still widely unknown. Content goes here… Outcome… Thus this women had two pregnancies in the left uterus which she lost but the pregnancy in the right uterus which was the bigger uterus resulted in a successful term pregnancy.She was given an appointment for ultrasound of the kidneys, and intravenous pyelogram as well a postnatal check in 6 weeks time. Fig.2.-Uteri marked with finger during caesarean section … … 7 months later she was reffered to the early pregnancy assessment unit 9+weeks pregnant, but this time ultrasound showed pregnancy in the right uterus corresponding to the gestational age by LMP. As the cervix was short 2cm in length a cervical suture was inserted at 12+ weeks of gestation. Detail scan of the fetus was normal and the growth was acceptable. Inj.Primulut 250mg weekly was prescribed to continue till 34 weeks of pregnancy. Her pregnancy progressed to 26 weeks of gestation when she was admitted in preterm labour and was treated with Tractocile (oxytocin antagonist) and 2 doses of betamethasone 24hrs apart was given intramuscularly. She was hydrated with normal saline and Diclofenic suppository 100mg was given for pain relief. Conservative treatment was planned as she did not show signs of impending labour.She was started on clexane 40 mg as she restricted mobilization. Fetal movement chart and daily cardiotocograph and 2-3 weekly growth scans were done to reassure and assess growth .At 32 weeks she went home and was seen regularly in the antenatal clinic.At 37 weeks of gestation cervical suture was removed and the patient wished for a vaginal delivery. The pelvis was assessed and the vagina and scarring to assess its stretchability. Cervix was central and 2cm in length os tightly closed .After discussion with the patient the pros/cons of vaginal /elective caesarean section, it was decided to have a short trial of labour with prostaglandin induction and if not in labour after two doses then for emergency caesarean section.As the Bishops score remained poor we proceeded for an emergency caesarean section under spinal anaesthesia. Her haemoglobin concentration was 10gm% and blood group was A+ve.She had blood pressure 130/80mmHg. Her urine sample showed absence of albumin and sugar.Abdomen was opened by transverse incision in layers and we observed two uteri with intervening thick connective fibrous band in between them. On the left side was a non-pregnant uterus,which was lying anterior and to the left side of the pregnant uterus.A live baby boy presenting by cephalic,was extracted out by lower segment caesarean section, with good apgar score,weighing 2.400 kg.The lower segment was well formed and the estimated blood loss was only 400mls.After closing the right uterus,we took snaps of both the uteri having separate fallopian tube and ovary shown in the figure below. She made a good postoperative recovery and went home with the baby on 5th postoperative day. Uterus didelphys as is the case should not be confused with uterus bicornis bicollis. Although both have separate uterine cavities the walls of the uterus bicornis bicollis are still slightly joined together, but not just by a thin septate but rather by a thick uterus wall. In a uterus didelphys these are completely separate, and the two uterine cavities are not even partially joined as was the situation in the present case. Interestingly, in our present case report, this women had single pregnancy in her right uterus and gave birth to a baby by caesarean section which corroborates with the findings of studies earlier reported. Conclusively, we may also state that patients with uterus didelphys belong to a high risk group and deserve special prenatal care. Therefore it is of great importance for the clinical management of these cases that abnormalities of the reproductive tract are detected in an early stage .In the study of uterine abnormalities, ultrasound is used which is as reliable as laparoscopy or hysterosalpingography. References References. 1. Green LK, Harris RE, Uterine anamolies; frequency of diagnosis and associated obstetric compications. Obstet Gynecol, 1976,47(4):427-429. 2. Brody S. Double uterus with double pregnancy. Am J Obstet Gynecol, 1954, 67(1): 161-167. 3. Getts JS. Double pregnancy in a uterus duplex unicollis. Am J Obstet gynecol, 1967,97(2):277-278. 4. Fedele L,Ferazzi E, Dorte M, Vercelleni P, Candiani G. Ultrasonography in the different diagnosis of ‘double’ uteri. Fertil Steril 1988, 50(2): 361-364. 5. Suhail MF, Khan H, Suhail S.Congenital uterine anamoly: Pregnancy in a woman with bicornis bicollis uterus.Ind J Pract Doctors, 2008, 5(1):58-62. 6. Tortora JM. Uterus didelphysate J Med 1971,71(17):2089-2092. 7. Clarke GC. Uterus didelphus with a pregnancy in each horn. Case report.Br J ObstetGynecol, 1977, 84(9):720. 8. Brown DC, Nelson RF. Uterus didelphus and double vagina with a delivery of a normal infant from each uterus. Can Med Assoc J, 1967,96(11):675-677. 9. Kekkonen R, Nuutila M, Laatikainen T. Twin pregnancy with a fetus in each half of a uterus didelphys. ActaObstetGynacol Scan, 1991, &0(4-5):373-374. 10. Kanakas N, Boos R, Schmidt W.Twin pregnancy in the right horn of a didelphys uterus; a case report.Eur j ObstetGynecolReprod boil, 1989, 32(3): 287-292. .






















