Download
1 / 7
90 likes | 587 Views
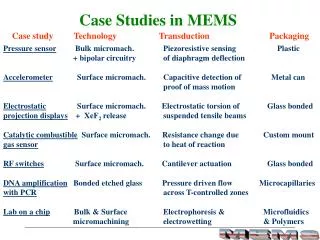
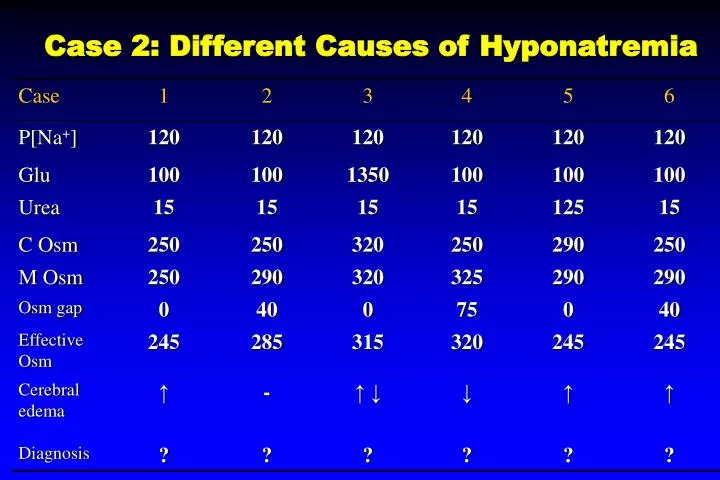
Case 2: Different Causes of Hyponatremia. Dilutional hyponatremia. True hyponatremia. Iso-osmotic. PseudohypoNa. Case 2: Different Causes of Hyponatremia. Hyponatremia 1. Calculated osmolality = 2 x Na + GLU/18 + BUN/2.8 2. measured osmolality 3. Osmolar gap = measure osm – calculated osm

E N D
Dilutional hyponatremia True hyponatremia Iso-osmotic PseudohypoNa
Hyponatremia 1. Calculated osmolality = 2 x Na + GLU/18 + BUN/2.8 2. measured osmolality 3. Osmolar gap = measure osm – calculated osm Increased osmolar gap >10 • Ethanol, methanol, ethylene glycol, mannitol • Pseudohyponatremia ( hyperproteinemia , hyperlipidemia )
Case 1 • True and acute hyponatremia with brain edema, not a chronic ,注意治療要快一點 • Case 2 • Iso-osmotic or pseudohyponatremia due to hyperproteinemia, hyperlipidemia • Nonsense osmolar gap, 間接性的關係 • 不用治療
Case 3. • Hyperosmotic hyponatremia due to hyperglycemia • 先算 Na decrease 1.6 meq/L for each increase glucose100mg/dl • mOsm increases in parellel with cosm, osm gap is zero • Effective osm is abnormally increased, 要先 r/o risk of brain edema • Treat hyperglycemia • Case 4 • Hyperosmotic hyponatremia due to mannitol • Mannitol is non sodium particle • Cosm 裏面 mannitol 沒有算進去 , abnormal low value of Cosm and increased osm gap • 有無 brain edema 要看 effective osm, not sodium • cerebral edema 用 mannitol 治療後 Brain cell volume 變 relatively 小
Case 5 • True hyponatremia due to elevated BUN , renal insufficiency • Mosm and Cosm 裏面 BUN算進去. The OG is Zero • Urea is ineffective osmole • Effective osm is low, hyponatremia 是有意義的, 有 risk of cerebral edema, • Treatment 快 or慢 depend on condition Case 6 • True hyponatremia, due to use of glycine in TURP or bladder irrigation , methanol, ethanol ingestion, retained particle, 有 osm gap • Low effective osmolality is increased risk of cerebral edema • Treatment is urgent