Download
1 / 108
1.1k likes | 1.3k Views
25. P A R T A. The Urinary System. Kidney Functions. Filtration – over 200 liters of blood filtered daily , allowing toxins, metabolic wastes, and excess ions to leave the body in urine Regulates fluid & electrolyte balance Assists with blood acid – base balance

E N D
25 P A R T A The Urinary System
Kidney Functions • Filtration – over 200 liters of blood filtered daily, allowing toxins, metabolic wastes, and excess ions to leave the body in urine • Regulates fluid & electrolyte balance • Assists with blood acid – base balance • Gluconeogenesis during prolonged fasting • Production of renin to help regulate blood pressure and erythropoietin to stimulate RBC production • Activation of vitamin D • Produces some thrombopoietin
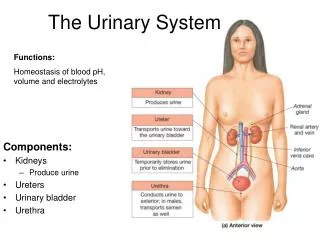
Other Urinary System Organs • Urinary bladder – provides a temporary storage reservoir for urine • Paired ureters – transport urine from the kidneys to the bladder • Urethra – transports urine from the bladder out of the body
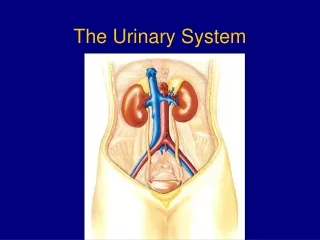
Urinary System Organs Figure 25.1a
Kidney Location and External Anatomy • Approximate size 12 x 6 x 3 in centimeters • Approximate weight 150 grams • The kidneys lie in a retroperitoneal position in the superior lumbar region – generally T12 – L3 – thus some protection from ribs 11 and 12 • The right kidney is lower than the left because it is crowded by the liver • The lateral surface is convex; the medial surface is concave • The renal hilus leads to the renal sinus • Ureters, renal blood vessels, lymphatics, and nerves enter and exit at the hilus
Layers of Tissue Supporting the Kidney • Renal capsule – fibrous capsule that prevents kidney infection • Adipose capsule – fatty mass that cushions the kidney and helps attach it to the body wall • Renal fascia – outer layer of dense fibrous connective tissue that anchors the kidney PLAY InterActive Physiology ®: Anatomy Review, page 4
Kidney Location and External Anatomy Figure 25.2a
Internal Anatomy (Frontal Section) • Cortex – the light colored, granular superficial region • Medulla – exhibits 6 – 12 cone-shaped medullary (renal) pyramids separated by columns • Each renal pyramid has a tip called the renal papillae which is perforated by 20 or so openings of the ducts of Bellini • The medullary pyramid and its surrounding capsule constitute a lobe (each kidney generally has between 6 to 12 lobes) • Collecting System – begins with minor calyx • Each renal papillae is covered by a cup like structure known as the ostium of the Minor Calyx ( thus for every lobe of the kidney there is a minor calyx.
Internal Anatomy • Several minor calyces join together to form a major calyx. • The major calyces join together to form the renal pelvis • Urine flows through the renal pelvis into a ureter • From the ureter urine enters the urinary bladder InterActive Physiology ®: Anatomy Review, page 6 PLAY
Internal Anatomy Figure 25.3b
Blood and Nerve Supply • Approximately one-fourth (1200 ml) of systemic cardiac output flows through the kidneys each minute • Arterial flow into and venous flow out of the kidneys follow similar paths • The nerve supply is via the renal plexus. The renal plexus consists of unmyelinated sympathetic fibers that travel with the arterial supply. The cell bodies are located in the aortic and celiac plexuses. • Lymphatic supply to kidney poorly understood
Renal Vascular PathwayAorta renal artery Anterior and Posterior division of renal artery 5 segmental arteries (do not anastomose) Lobar arteries Interlobar arteriesArcuate arteries Interlobular arteries Afferent arterioles Glomerulus Efferent arterioles Peritubular Cap and Vasa Recta (arteriolae rectae and vena rectae) Arcuate veins (if from the vena rectae) – deliver into stellate veins then to interlobular veins if from cortical peritubular capillaries then to arcuate veins Interlobar veins renal veins Figure 25.3c
Capillary Beds of the Nephron • Every nephron has two capillary beds • Glomerulus • Peritubularcapillaries OR Vasa Recta • Each glomerulus is: • Fed by an afferent arteriole • Drained by an efferent arteriole
Capillary Beds • Peritubular beds are low-pressure, porous capillaries adapted for absorption that: • Arise from efferent arterioles • Cling to adjacent renal tubules • Empty into the renal venous system • Vasa recta – long, straight efferent arterioles of juxtamedullary nephrons
Capillary Beds Figure 25.5a
Functional Unit of the Kidney – Uriniferous tubulesFunctional Unit – least amount of anatomy to explain the entire physiology The uriniferous tubules consists of the nephron (generally referred to as the functional unit of the kidney) and a portion of the collecting duct The nephron consists of a) the glomerulus b) Bowman’s capsule c) the proximal convoluted tubule d) the Loop of Henle e) the Distal convoluted tubule and f) the connecting tubule The combination of the glomerulus and Bowman’s capsule constitutes the “Renal Corpuscle” • Renal corpuscle – the glomerulus and its Bowman’s capsule • Glomerular endothelium – fenestrated epithelium that allows solute-rich, virtually protein-free filtrate to pass from the blood into the glomerular capsule
The nephrons are all located in the cortical region of the kidneys – but they are at three levels in the cortex . The outer cortical nephrons, the mid-cortical nephrons and the inner cortical nephrons termed the “Juxtamedullary nephrons – approximately 15% of nephrons. The juxtamedullary nephrons have the longest loops of Henle (associated with concentrating the urine). Each kidney has approximately 1 – 1.3 million nephrons. • The renal corpuscle which consists of the glomerulus and Bowman’s capsule is where the actual filtration of the blood occurs.
Nephrons • Cortical nephrons – 85% of nephrons; located in the cortex • Juxtamedullary nephrons: • Are located at the cortex-medulla junction • Have loops of Henle that deeply invade the medulla • Have extensive thin segments • Are involved in the production of concentrated urine
The Nephron Figure 25.4a, b
Renal Corpuscle • The glomerulus is a tuft of fenestrated capillaries that allows a filtrate of the blood to enter Bowman’s capsule • Between the capillary loops of the glomerulus are Mesangial cells (intraglomerular) and some located at the vascular pole of the renal corpuscle (extraglomerular). • The intraglomerular Mesangial cells are a) phagocytic thus cleaning the filter b) contractile in that they have receptors for vasoconstrictors like angiotensin II c) help support the capillaries in regions where the visceral layer of Bowman’s capsule does not come in contact with the capillaries. • The extraglomerular mesangial cells are connected by gap junctions and may serve as a communication between macula densa and granular cells.
Three jobs to make urine • 1. Filtration – removal of substances from the blood at the filter (renal corpuscle) • 2. Reabsorption – returning much of the filtrate (minus most of the waste) back into the blood – reason – too much has been filtered • 3. Secretion – active transport of substances absolutely needed to filtered into the kidneys in areas after the filter
Mechanisms of Urine Formation • Urine formation and adjustment of blood composition involves three major processes • Glomerular filtration • Tubular reabsorption • Secretion Figure 25.8
Filtration - Composition of the Filter • The capillary fenestra – range between 70 – 90 nm – this prevents the formed elements of the blood (except a few WBCs that can perform diapedesis) from being filtered along with any macromolecules (some of the plasma proteins) whose effective size exceeds the diameter of the fenestra (atomic mass exceeds 70,000 AMUs) • The Basal Lamina (300nm thick) consists of three layers the lamina densa (has type IV collagen) in the middle surrounded by a lamina rara on each side (lamina rara has the negatively charged substance heparin sulfate). The Lamina Densa traps larger proteins > 69,000 AMU and the negatively charged Lamina rara impedes negatively charged molecules from leaving (most of the plasma proteins are negatively charged).
Filter Continued Anatomy of the Glomerular (Bowman’s) Capsule • Bowman’s capsule is composed of two layers – the internal visceral layer that actually abuts the glomerular capillaries. This layer consists of modified, branching epithelial podocytes. • Extensions of the octopus-like podocytes terminate in foot processes – primary processes and secondary processes (pedicels) • Filtration slits – 20 – 40 nm width openings between the foot processes that allow filtrate to pass into the capsular space
Filtration Slits are covered • The filtration slits are covered by a 6nm thick slit diaphragm which extends between the secondary pedicels • The slit diaphragm has circular pores that are approximately 3-5 nm in diameter • As a result of the filtration anatomy – substances smaller than 3 nm easily transverse the anatomical filter – those larger than 5 nm generally do not cross . Examples of these substances would be water, electrolytes, glucose, amino acids, small proteins, urea, uric acid, creatinine and others
Glomerular Filtration • Principles of fluid dynamics that account for tissue fluid in all capillary beds apply to the glomerulus as well • The glomerulus is more efficient than other capillary beds because: • Its filtration membrane is more permeable • Glomerular blood pressure is higher • It has a higher net filtration pressure • Plasma proteins are not filtered and are used to maintain oncotic pressure of the blood
Net Filtration Pressure (NFP) • The pressure responsible for filtrate formation • NFP equals the glomerular hydrostatic pressure (HPg) minus the oncotic pressure of glomerular blood (OPg) combined with the capsular hydrostatic pressure (HPc) • 10 mmHg = 55 mm Hg – (30 mmHg + 15mmHg) Usual pressures in most capillaries are: • 10 mmHg = (35mmHg + 1mmHg) – (26 mmHg) NFP = HPg– (OPg+HPc)
Comparison of NFP • NFP = pressure out of capillary – pressure into • Forces out = MAP at capillary + Interstitial Fluid Osmotic Pressure • Forces into = Interstitial Hydrostatic Pressure + Blood Osmotic Pressure • MAP at general Capillary – 30 - 35 mmHg but at glomerulus 55 mmHg - why? efferent arteriole narrower than afferent arteriole – won’t blow out capillary due to being wrapped by podocytes • Interstitial Fluid Osmotic Pressure 1 mm Hg in most capillaries – 0 mmHg in kidney due to non-filtration of the plasma proteins
Blood osmotic pressure 26 mmHg in most capillaries but 30 mmHg in Glomerulus due to increased concentration of plasma proteins due to non-filtration • Interstitial fluid hydrostatic pressure 0 mmHg in most tissues but 15 mmHg in kidney due relative lack of lymphatics and the narrowness of the Proximal Convoluted Tubule compared to Bowman’s space.
Vascular Resistance in Microcirculation • Afferent and efferent arterioles offer high resistance to blood flow • Blood pressure declines from 95mm Hg in renal arteries to 8 mm Hg in renal veins (in most other venules and veins it drops to 10 – 15 mm Hg) • The reason is due to the two arteriole anatomy- one arteriole coming into the glomerulus (afferent arteriole) and one coming out (efferent arteriole) – the combination of these two resistors significantly drops the pressure
Vascular Resistance in Microcirculation • Resistance in afferent arterioles: • Protects glomeruli from fluctuations in systemic blood pressure – if blood pressure gets to high – vasoconstrict so as to not blowout the glomerular capillaries – if to low vasodilate to let more blood into glomerulus so Glomerular Filtration Rate does not drop. • Resistance in efferent arterioles: • Reinforces high glomerular pressure – vasoconstriction gives a better back pressure • Reduces hydrostatic pressure in peritubular capillaries – this provides a better suction pressure in the peritubular capillaries for reabsorption of water
Renal Blood Flow (RBF) – how much whole blood flows to both kidneys in a minute – generally about 25% of cardiac output – average 1250 ml per minute • Renal Plasma Flow (RPF)– since the glomerulus filters out the formed elements – then really what goes into Bowman’s capsule is filtered plasma RPF = RBF(1 − HCT) (Determined by Clearance of PAH) • Glomerular Filtration Rate (GFR) – what is the amount of the plasma that is filtered in one minute – on average approximately 125 ml per minute (Determined by Clearance of Creatinine) • Clearances to be Discussed Later • Filtration Fraction – what percentage of plasma is filtered in a minute FF = GFR / RPF x 100
Regulation of Glomerular Filtration • Three mechanisms control the GFR • Renal autoregulation (intrinsic system) inside kidney • Neural controls (Extrinsic) • Hormonal mechanism (the renin-angiotensin system)- Extrinsic THESE WILL BETTER BE DISCUSSED LATER
The start of Reabsorption in the Renal Tubule • The ultra-filtrate of the blood now enters the first tubule (small tube) which is the Proximal convoluted tubule (PCT) – its walls are lined with cuboidal epithelial cells with numerous microvilli (increase surface area for reabsorption) and mitochondria (lots of active transport – both primary and secondary) • The speed at which the glomerulus filters blood is termed the Glomerular Filtration Rate which on average is 125 ml per minute so in a day you put on average over 200 + liters of filtrated blood into the kidneys • You only have 3 – 6 liters of blood so you can see that you must reabsorb most of your fluid back into the blood stream • Thus the main job of the PCT is Reabsorption of much of your ultrafiltrate of the blood
Reabsorption in the PCT • Generally 100% of glucose, amino acids, lactate, vitamins, and other non-waste organic substances • 80% of filtered bicarbonate • 65% of sodium, water • 60% of chloride • 55% of potassium • Almost all of the uric acid and 50% of the urea reabsorbed but later secreted
Tubular Reabsorption • Two routes – transcellular or paracellular • Transcellular – through the cell • Paracellular – between the cells • Most travel by transcellular - transported substances move through three membranes • 1. Luminal and 2. basolateral membranes of tubule cells and 3. endothelium of peritubular capillaries • Ca2+, Mg2+, K+, and some Na+ are reabsorbed via paracellular pathways Chloride also is reabsorbed paracellular in the proximal part of PCT and transcellular in Distal part • The epithelial cells are linked by leaky tight junctions
Renal Tubule Figure 25.4b
Sodium Reabsorption: Primary Active Transport • Sodium reabsorption is almost always by active transport • Na+ enters the tubule cells at the luminal membrane • Is actively transported out of the tubules by a Na+-K+ ATPase pump
Sodium Reabsorption: Primary Active Transport • From there it moves to peritubular capillaries due to: • Low hydrostatic pressure (as a result of narrower efferent arteriole giving resistance) • High osmotic pressure of the blood (as a result of increased concentration of plasma proteins – remember they were never filtered in glomerulus but water was taken out – thus increase in effective concentration of these proteins • Na+ reabsorption provides the energy and the means for reabsorbing most other solutes
Reabsorption by PCT Cells • Active pumping of Na+ drives reabsorption of: • Water by osmosis, aided by water-filled pores called aquaporins (obligatory water reabsorption) • Aquaporins I are permanent residents of the PCT epithelial cells unlike in the DCT where they will be controlled by antidiuretic hormone • Cations and fat-soluble substances by diffusion- as the water leaves the concentration of cations and fat soluble substances increase thus forcing diffusion of them – an example of solute following solvent • Organic nutrients and selected cations by secondary active transport
Small proteins that mistakenly get filtered are removed by pinocytosis • Secondary Transporters cause reabsorption of the most of the organic substances like glucose, amino acids, lactic acid, sulfate and phosphate • The Secondary Transport substances are limited by a Transport Maximum (Tm) – the amount removed cannot exceed the amount of transport carriers – another term for this is to exceed renal threshold • H+ removal will be discussed later in my renal acid- base discussion
Non-reabsorbed Substances • A transport maximum (Tm): • Reflects the number of carriers in the renal tubules available • Exists for nearly every substance that is actively reabsorbed • When the carriers are saturated, excess of that substance is excreted – exceeds Tm or also termed exceeds renal threshold
Nonreabsorbed Substances • Substances are not reabsorbed if they: • Lack carriers (secondary transport) • Are not lipid soluble • Are too large(and water soluble) to pass through membrane pores (thus electrolytes pass through membrane pores) • Creatinine is an important non-reabsorbed substance (but its non- reabsorption is advantageous in medicine in that it can be used to determine the Glomerular Filtration Rate GFR rate determination – discussed later