Download
1 / 32
380 likes | 955 Views
Double Inlet Ventricle. Seoul National University Hospital Department of Thoracic & Cardiovascular Surgery. Double Inlet Ventricle. Definition

E N D
Double Inlet Ventricle Seoul National University Hospital Department of Thoracic & Cardiovascular Surgery
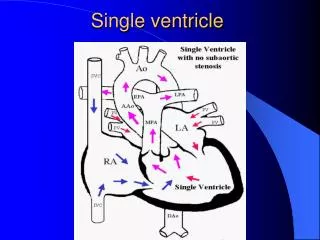
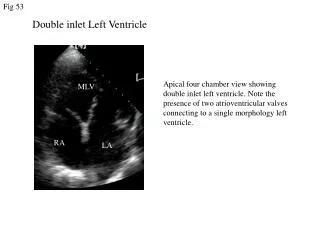
Double Inlet Ventricle • Definition A congenital cardiac malformation in which both atria connect to only one ventricular chamber by either two separate atrioventricular valves or a common AV valve Single ventricle, univentricular AV connection • History Holmes : Solitary ventricular chamber in 1824 Rokitansky : Double inlet left ventricle in 1875 Taussig : Single ventricle in 1939 Van Praagh : Clear definition of this entity in 1964 Muller & Damman ; PA banding for single ventricle in 1952 Mayo Clinic : Septation on single ventricle
Double Inlet Ventricle • Pathophysiology • A single functional ventricle receives both systemic and pulmonary venous return via right- & left-sided atrioventricular valves or a single common valve, resulting in mixing of oxygenated & deoxygenated blood and , hence, systemic arterial hypoxemia. • This defect is also associated with excessive or inadequate pulmonary blood flow, depending on whether there is obstruction to pulmonary flow (e.g., pulmonary stenosis/atresia).
Double Inlet Ventricle • Morphology • Ventricular mass Main( dominant) chamber, Nondominant chamber, Bulboventricular foramen • Atria Any types of atrial situs can be present • Atrioventricular connection Usually two AV valves, Valves or common valve overriding in 20 % of cases • Ventriculoarterial connection • Conduction tissue • Coronary arteries
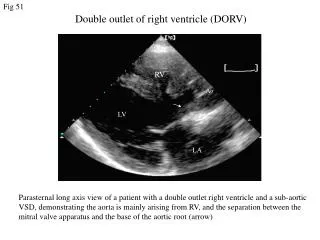
Types of Double Inlet Ventricle 1.Double inlet LV with left-sided rudimentary RV & discordant ventriculoarterial connection {S,L,L} 2. Double inlet LV with right-sided rudimentary RV & concordant ventriculoarterial connection ({S,D,S} : Holme’s heart) 3. Double inlet LV with right-sided rudimentary RV & discordant ventriculoarterial connection {S,D,D} 4. Double inlet and double outlet LV 5. Double inlet and double outlet RV 6. Double inlet RV with concordant ventriculoarterial connection 7. Solitary ventricle of intermediate morphology
Frequent Double Inlet Ventricle • DILV with left rudimentary RV & discordant VA connection {S,L,L} * Most frequent type (50%) * Restrictive VSD is frequent : subaortic stenosis, CoA, IAA * Subpulmonic obstruction : favorable clinical course * Frequent stenosis or hypoplasia of AV valve • DILV with right rudimentary RV & concordant VA connection {S,D,L} * Less than 10% * Usual atrial arrangement * Frequent right AV valve straddling and overriding * Usually restrictive VSD • Double inlet and double outlet right ventricle * About 5% * Usual atrial arrangement, or right isomerism * PS or PA and TAPVR
DILV (1) Morphologic LV
DILV (2) Morphologic RV
Double Inlet Ventricle • Connections * Atrioventricular • concordant • discordant : frequent • ambiguous • * Ventriculoarterial • concordant • discordant : frequent (60-80%)
Double Inlet Ventricle • Associated cardiac anomalies • Subaortic stenosis (restrictive BVF or VSD) • Pulmonary stenosis (subpulmonary stenosis) • Pulmonary atresia • Patent ductus arteriosus • AV valve stenosis, hypoplasia, straddling, overriding • IAA, CoA, aortic arch hypoplasia
Double Inlet Ventricle • Natural History • Incidence 3% of CHD M : F = 2.5 : 1 • Estimated overall survival without treatment • 1) Not entirely accurate • 2) Less risk of death during neonatal & infant period • 3) 57%, 45% remain alive at 1, 5 years • 4) Acidosis & low cardiac output is a severe risk factor • 5) Systemic outflow obstruction is strong risk factor
Clinical Features & Diagnosis • 1. Clinical features are governed by the morphology & • associated lesions • 2. Variable according to following anomalies • (TAPVR, PS, PA, subaortic obstruction, CoA, IAA, • unobstructed pulmonary blood flow) • 3. Pulmonary blood flow • 1/3 : decreased • 2/3 : increased • small % : balanced • 4. Electrocardiogram & chest radiography • 5. Echocardiography & cineangiography • 6. CT angiography & MRA
Systemic Outflow Obstruction • Initial Palliation • Pulmonary artery banding & CoA repair • Norwood & DKS type operation • Palliative arterial switch operation • Alternative surgical approaches ; PAB, CoA repair, enlargement of BVF, Apical LV-aortic conduit, Transplantation
Systemic Outflow Obstruction • Surgical treatment of subaortic stenosis in functional single ventricle
Operative Management • Techniques • Septation • * At any age or in patients with increased PVR, or after • palliative procedure • * Usually in {S,L,L} type single ventricle • * Some of {S,L,D} with arterial switch operation (without PS) • * High mortality and complications • (complete heart block, residual VSD, A-V valve regurgitation, • sudden death) • Fontan operation • * Usually done around 2 years old • * After banding or systemic-pulmonary artery shunt
Fontan Operation • Right AV valve may be closed as part of Fontan-type • repair in double inlet left ventricle
Septation Operation • Septation is performed through right atrial approach, • best illustrated through fishmouth incision in the ventricle
Operative Management • Surgical results • Septation • * Recently improved hospital mortality (10 - 30%) • * Late functional result : good • Fontan-type procedure • * Nearly same early and late result as other types of CHD • Palliative procedure • * Pulmonary artery banding • * Systemic-pulmonary shunt • * Atrial septectomy
Suitable Septation Operation • Apparently, 20-25% of patients with double inlet ventricle are suitable at birth for septation • Somewhat, not severely, enlarged dominant ventricle • Two reasonable competent and nonstenotic AV valves with little or no overriding or straddling • There should be little or no pulmonary or systemic outflow obstruction • Septation should be performed during the first year or two of life • Consideration should be given to a two-stage approach, to minimize the probability of producing complete heart block
Indications of Operation • Primary considerations in managing the patients with double inlet ventricle of any type are (1) their suitability for septation, Fontan operation, or cardiac transplantation and (2) prevention of additional complicating conditions such as subaortic stenosis or pulmonary arterial stenosis
Atrial Isomerism • Definition • Atrial isomerism is a condition in which the right-sided and left-sided atria, normally morphologically different, are morphologically similar. • Atrial isomerism is a subset of situs ambigus, a condition in which usually asymmetric bodily structures tend to be symmetric.
Morphology of Atrial Isomerism • Bilateral right or left atria • Conduction system • Anomalies of systemic venous connection • Anomalies of pulmonary venous connection • Atrioventricular connection • Atrioventricular septal & other atrial septal defect • Ventricular morphology and VSD • Pulmonary outflow tract • Ventriculoarterial connection • Other coexisting cardiac anomalies
Clinical Features & Diagnosis • There are no other clinical features specific to atrial isomerism • Asplenia is associated with an increased number of Howell-Jolly bodies • Clinical features depend, therefore, on other cardiac anomalies that may present. • Almost all with right atrial isomerism have sinus rhythm, & complete heart block coexist in 10% of left artrial isomerism, but rare in right atrial isomerism • Echocardiography • Cardiac catheterization
Natural History • Determined primarily by details of cardiac structures and nature of coexisting cardiac anomalies. • However, atrial isomerism itself may contribute to natural history because of its association with neonatal complete heart block and sometimes neonatal death • Right atrial isomerism is often accompanied by asplenia, a condition believed to render the patient susceptible to infection, particularly pneumococcal. • Left atrial isomerism is often accompanied by a polysplenia and a high prevalence of extrahepatic biliary atresia
Operative Indications & Technique • Need for surgical treatment is dictated by associated cardiac anomalies, not by atrial isomerism • Technique • Cardiopulmonary bypass • Intracardiac repair • Complex atrial baffle • Fontan type repair • Palliative operations
Results of Surgical Treatment • Overall survival is better with left, compared to right atrial isomerism • Survival is better when a biventricular repair is undertaken • Although, overall outcomes of isomerism have been poor, results have improved substantially over time • In left atrial isomerism, one third possibly received by biventricular repair, one third by Fontan, no palliation in others. • In right atrial isomerism, both short and long-term outcomes are poor, and biventricular repair is possible in few patients.
Incremental Risk Factors for Death • Left atrial isomerism • Lower birth weight • Single ventricle • Gastrointestinal malformation • Biliary atrsia • Congenital AV block • Coarctation of aorta. • Right atrial isomerism • Absence of pulmonary outflow obstruction • Presence of AV valve anomaly • Presence of obstructed pulmonary veins