Download
1 / 32
330 likes | 729 Views
Double Switch Operation for Failing Systemic Ventricle. Yong Jin Kim, M.D. Department of Thoracic & Cardiovascular Surgery Seoul National University Hospital. Introduction.

E N D
Double Switch Operation for Failing Systemic Ventricle Yong Jin Kim, M.D. Department of Thoracic & Cardiovascular Surgery Seoul National University Hospital 2001.7
Introduction • Conventional managements of AV discordant heart ( Atrial switch operation in TGA) place the morphologic right ventricle & tricuspid valve in the systemic position • The morphologic RV shows significant incidence of progressive ventricular dysfunction & TV regurgitation • Double switch operation (Conversion switch operation) as an alternative in selected patients 2001.7
Congenitally Corrected Transposition of Great Arteries • 1. Incidence 0.5% of CHD, slightly male predominating • 2. Heart block • 1) Complete heart block • 5-10% at birth, 10-15% in adolescence, 30% in adult • 2) 1st or 2nd degree A-V block ; 40 - 50% at birth • 3) 40% retain normal PR interval & QRS through their lives • 3. Ventricular function Not truly normal, but sufficiently good in most • Tendency to deteriorate after 2nd –3rd decade of life. • 4. Coexisting cardiac anomalies • VSD, PS, left A-V valve incompetence ( tricuspid ) 2001.7
Characteristics of Both Ventricles 1. Ventricle shape Cylindric vs. crescent-shaped cavity 2. Contraction pattern • Concentric vs. bellow-like contraction 3. Pumping action • Pressure pump vs. low pressure-volume pump • 4. Coronary artery supply • Two system vs. one system 5. Embryology • Primitive ventricle vs. bulbus cordis 6. Papillary muscles • Two papillary vs. small & numerous (septophylic) 2001.7
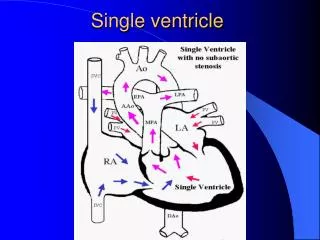
Congenitally Corrected TGA 2001.7
Classic Operative Indications of CC-TGA • The presence of corrected TGA is not an indication • for a reparative operation • 1. Ventricular septal defect · same as normal heart • 2. VSD & Important PS • · same as TOF • 3. Left-sided tricuspid incompetence • · same as mitral incompetence • 4. Complete heart block 2001.7
Classic Operation of CC-TGA • 1. Repair of ventricular septal defect • 2. Repair of coexisting VSD & PS • · Extracardiac conduit • · Without extracardiac conduit • 3. Correction of incompetent tricuspid valve • · Repair ( annuloplasty ) • · Replacement • 4. Fontan-type repair • Straddling, A-V canal , hypoplastic ventricle 2001.7
“ Classic” Repair of Congenitally Corrected TGA and VSD(Termignon JL, et al. Ann Thorac Surg 1996) • From 1974 to 1994, 52 CC-TGA patients CC-TGA & VSD + LVOTO (Group I) : 37 CC-TGA & Isolated VSD (Group II) : 15 • Tricuspid plasty or replacement 1 (3%) in group I, 8 (53%) in group II • Overall operative mortality : 15% (8/52) Incidence of postop. AV block 27% (14/52) Redo tricuspid valve plasty or replacement in 12 The operative mortality , the incidences of TVR & AV block are high Secondary heart failure is frequent 2001.7
Tricuspid Regurgitation & RV Dysfunction in CC-TGA • High risk of TR development by the 3rd decade of life (20 to 50%) • Most important risk factor for death after classic repairs • Measurable deterioration of RV within 3 years of classic repairs • RV dysfunction appears to be almost secondary to long-standing TR ( Prieto, et al. Circulation.1998 ) 2001.7
Major Problems after Atrial Switch Operation in TGA • Right ventricular failure 7-10% per 10 years , high with VSD closure • Tricuspid regurgitation • Rhythm disturbance 1/3 of patients lost sinus rhythm after 10 years & atrial flutter is risk factor for late death 2001.7
Morphologic RV after Atrial Switch Operation • Nature of right ventricle • One coronary ventricle • One conduction radiation • Without well-balanced papillary muscle • Not suitable to systemic ventricular function • Tricuspid regurgitation • Stretching of originally noncircular tricuspid ring Poorly supported tricuspid annulus – RV dysfunction may induce important TR 2. Damage of TV valve as a result of VSD patching 3. Failure of systolic leaflet coaptation 2001.7
Surgical Management for Failing Systemic RV • Double switch operation Correction of AV and VA discordance simultaneously • Senning(Mustard) + ASO • Senning(Mustard) + Rastelli • Senning(Mustard) + REV • Conversion switch operation • Previous atrial switch take-down & ASO 2001.7
Surgical Considerations • Left ventricular outflow tract • Status of atrioventricular valves • Ventricular size & its function • Heart block & arrhythmias • Patterns of coronary arteries • Status of atrial switch operation • Technical problems for ASO • LV training & timing of operation 2001.7
Proposed Patient Selection Criteria • Unobstructed LV-PA & RV-Ao connections • Balanced ventricular & AV valve sizes • Septatable heart, without AV valve straddling • Translocatable coronary arteries • Current LV/RV pressure ratio greater than 0.7 • Competent mitral valve with good LV function (Karl TR, et al. ATS 1997) 2001.7
Preparation for Systemic Left Ventricle • Naturally occurring preparation • Pulmonary artery banding • Age • Banding (LV retraining) duration • Preoperative selection criteria • Age • Wall thickness • LV/RV pressure ratio 2001.7
Senning Procedure 2001.7
Mustard Procedure 2001.7
Senning plus ASO 2001.7
Conversion Switch Operation 2001.7
Senning Plus Arterial Switch Operation for Congenitally Corrected Transposition (TR Karl, et al. Ann Thorac Surg 1997) • From 1989 to 1996 • 14 Senning + ASO : age 0.5 to 120mo • 1 hospital mortality • Actuarial survival beyond 10 months : 81% • Median grade of TR : preop ¾ to ¼ postop • Normal RV function : 11/12 current survivors 2001.7
Results of the Double Switch Operation in the Current Era (Imamura, et al. Ann Thorac Surg 2000) • From 1993 to 1998 • 22 Double Switch Operations : 3mo to 55yrs • Senning & ASO : 10 • Senning & Rastelli : 12 • No early and late Mortality • Epicardial pacemaker insertion in 2 • Significantly improved degree of TR with normal LV and RV function 2001.7
Systemic Right Ventricular Failure after Atrial Switch Operation: Midterm Results of Conversion into an Arterial Switch (Daebritz SH, et al. Ann Thorac Surg 2001) • 4patients age 38 to 59 months of RV failure underwent arterial switch operation • Previous operation : Senning & VSD closure • 1 late death(43.5 mo) due to LV dysfunction • Survivors : improved FS, NYHA class I – II • Alternative to cardiac transplantation in children • Long-term morbidity caused by rhythm disturbance 2001.7
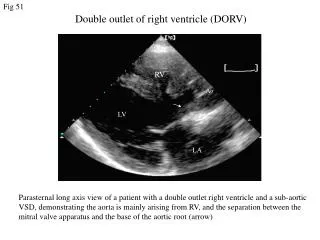
Experience in SNUCH • From 1990 to 2001 ( 21 patients ) • 20 double switch operations • 1 conversion switch operation • Age : ranged 1 month to 16 years (mean 46months) • M : F = 12 : 9 • Dx : CC-TGA (with VSD, PS or PA) – 18 DORV(l–loop), PS, VSD – 2 d-TGA, VSD – 1 ( Conversion switch after Senning ) 2001.7
Experience in SNUCH • Preoperative procedures (13 ) • Pulmonary artery banding : 2 • LMBTS : 3 • RMBTS : 1 • LMBTS + RMBTS : 2 • VSD closure : 2 • Atral septostomy : 1 • PPM insertion : 1 • RV-PA conduit : 1 2001.7
Experience in SNUCH • Operative techniques in 21 patients • Senning + ASO : 6 • Senning + Rastelli : 9 • Mustard + ASO : 1 • Mustard + Rastelli : 1 • Senning + REV : 2 • Mustard + REV : 1 • * 1 conversion arterial switch operation after Senning & PAB 2001.7
Experience in SNUCH • Overall operative mortality : 6 / 21 (28.5%) • Number of death according to period • 1990 - 1993 : 5 / 10 (23.8%) in initial period LCOS 4 , sepsis 1 * 3 early myocardial failure • 1994 - 2001 : 1 / 11 ( 4.8%) Sepsis 1 2001.7
Experience in SNUCH • Complications • AV block : permanent pacemaker in 3 • Chylothorax in 4 • Reoperation in 3 • Senning pathway reaugmentation • Redo Rastelli op. d/t residual PS • Conduit change with Homograft 2001.7
Experience in SNUCH • Overall outcomes in survivors - Postoperative TR : all survivors in minimal or grade I - Preserved ventricular function : all in NYHA functional class I or II 2001.7
Operative Procedure 2001.7
Conclusion • TR and the subsequent RV dysfunction represent the major risk factor for CC-TGA patients. • Double switch operation in selected patients in optimal anatomic & physiologic subsets has encouraging early outcomes with its theoretical advantages. • Conversion switch operation can be performed with an acceptable risk , and may provide long-term survival if adequate patient preparation is warranted. 2001.7