Download
1 / 38
400 likes | 663 Views
RECTAL CARCINOMA. ELSHAMI ELAMIN, MD Central Care Cancer Center Newton, KS-USA. RISK FACTORS. Dietary factors Fat ? Fiber ? Calcium ? Vitamins (E, -carotene) Aspirin/NSAIDs (Cox inhibitors) Sulindac reduces polyps in FAP pts Aspirin lower risk of CRC. RISK FACTORS.

E N D
RECTAL CARCINOMA ELSHAMI ELAMIN, MD Central Care Cancer Center Newton, KS-USA
RISK FACTORS • Dietary factors • Fat • ? Fiber • ? Calcium • ? Vitamins (E, -carotene) • Aspirin/NSAIDs (Cox inhibitors) • Sulindac reduces polyps in FAP pts • Aspirin lower risk of CRC
RISK FACTORS • Genetic Factors • FAP(APC gene = Tumor suppressor gene) • 1-2% of CRC • Invasive cancer occurs at ~ 42Y • HNPCC (MMR mutations) • Hx of > 3 family members involving 2 generations with one diagnosed before age 50 • 4-6% incidence • Rt-sided cancer • Caused by defective DNA mismatch repair genes
Steps for Colorectal Carcinogenesis 1- Mutation at MCC and APC genes 2- K-ras oncogene activates adenoma to carcinoma 3- Mutation of p53 tumor suppressor gene
SCREENING • Patients with average risk • Asymptomatic • >50Y • No colorectal risk factors • FOBT (33% reduction in mortality) • Flexible sig (60-80% reduction in mortality) • Double-contrast BE • Colonoscopy (Gold standard)
Patients with increased Risk • First-degree relative with CRC or adenomatous polyps • FAP • F.H. of HNPCC • Adenomatous polyps • CRC • IBD
Hereditary CRC syndromesScreening and Management • FAP • Genetic counseling/gene testing • Is cost-effective • Genetic mutation not identified: • Flex sig at puberty and annualy • Colonoscopy if +ve sig • +ve FAP • Total colectomy
HNPCC (Lynch syndrome) • Lynch I: • No associated cancers • Lynch II: • Associated with ovarian, uterine cancers • Genetic testing • Difficult due to multiple mutations • MLH1, MSH2 mutations • Screening begin at 20Y and every 1-2Y • Genetically +ve: Consider colectomy/TAH/BSO
Work-up • Laboratory: • LFTs • CBC, Iron profile • CEA • Preoperative CT scan • Colon cancer: Adjacent organ invasion/Liver met • Rectal: Adjacent organ invasion/LN spread • For preop RT
MRI • Bowel wall penetration • MRI: 64%, CT: 62% • Sensitivity for LN met: 15-40% • Endorectal surface coil MRI for N1 • 72% specificity
Transrectal US • Evaluation for preop cheop/RT • Only 83-88% specific in separating T-T2 from T3-T4 • LN specificity • 28% for 5mm LN • 62% for 7mm
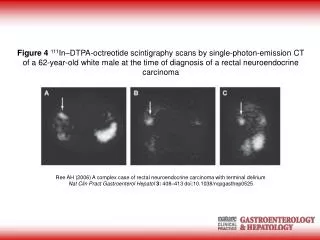
CEA scan • Coupled with standard CT • Can predict preop respectability
PET Scan • Staging • Restaging • 91% sensitivity, ~ 100% specificity for pelvic disease (CT: 52%, 80%) • 95% sensitivity for liver disease (CT 74%)
Staging • Dukes’ classification • Based on depth of invasion and LN • A: Limited to bowel wall • B: Extrarectal tissues • C: LN + • Modified Dukes’ (Astler-Coller system) • C1 and C2
TNM • Stage I: T1 (invade submucosa) A T2 (invade muscul propria) B1 • Stage II: T3 (invade through musc propria B2 into subserosa or nonperit. Tissue) T4 (perforate ves perit or B3 invade adjacent structure) • Stage III: N1 (1-3 pericolic/rectal) N2 (> 4) C N3 (along vascular trunk) • Stage IV: M1
Prognostic Factors • Adjacent tissue or vascular invasion • Nodal status • Micromets (<5mm) same as enlarged LN • 4 LN vs >4 • ? Cellular pathologic factors • S-phase, ploidy • Liver mets • Normal LFTs: 18 month med S • Elevated Bil: 6 wks med S
Prognostic Factors • CEA • Weak prognostic factor • Persistant CEA elevation = Residual dz • May increase initially during adjuvant • Not prognostic factors • Age, Sex, Tumor size
Rectal CaSurgical Treatment • Abdominal Perineal Resection (APR) • Permanent Colostomy • Sphincter Preservation
APR • Based on: • Rectal cancer spread via lymphatic pathways in proximal, lateral and distal direction • Decreases local recurrence • Improve survival • Permanent colostomy
APR • Candidates • Primary sphincter dysfunction • Tumor invading anal canal • High risk for local recurrence • Bulky disease • Poorly differentiated involving lower 1/3 • Direct extension into adjacent organs
Total Mesorectal Excision (TME) • Tumor spread into adjacent mesorectum • >2cm distal extension from the margin carries poor prognosis • Decreases local recurrence • Improve survival • Standard for mid and lower rectal cancers • Preserves pelvic autonomic nerve function
Local Excision • Lower 1/3 early rectal cancer (T1) • < 4 cm in diameter • Mobile lesion • Involve < 1/4 of circumference of bowel • Moderate to well differentiated • From 2 prospective Trials • T1 : Local excision alone • T2 : Local excision + CT/RT
Local Excision with RT • Indications • T2 • Lymphatic/vascular invasion • Poor histology • Positive margin • Fragmented resection
Endocavitary RT • Selection criteria • Distal lesion • No disease beyond bowel wall • No major extension to anal canal • T < 3x5 cm • Local failure • 5-20% • Salvage radical surgery
Low Anterior Resection (LAR) 1- Bowel divided at 5cm above rectal tumor 2- Ligation of superior hemorrhoidal artery 3- Total Mesorectal Excision (TME) for mid/lower rectal tumors 4- 11/2 - 2cm distal margin 5- Colo-Rectal anastomosis
Colonic J-Pouch • For low rectal cancer • To prevent incontinence/urgency
APR vs Sphincter Sparing Resections (SSR) in Mid-rectal cancers 5 Y S % APR SSR Mayo et al 69 72 Patel et al 56 64 Jones/Thomson 52 67 Williams/Johnston 62 74 • Local recurrence: APR 8%, SSR 11% (not significant)
Rectal Cancer • Incidence of local failure after resection • T1, T2N0: <10% • T3N0: 15-30% • T3N1: 35-50% • T3-T4N1: 60% • No successful salvage procedure
Pre-Operative RT • Improves local control (Several studies) • Improves OS (Only one study) • Downside • Overtreatment of T1, T2 • Use Transrectal US • Treatment of patient with hepatic mets • Use spiral CT
Locally Advanced Rectal Cancer • PreOp external RT + IntraOp RT • 67%5Y local control, 57% DFS • PreOp RT or Chemo/RT • 70-85% resectability and sphincter sparing surgery
Locally Recurrent Disease • Treatment options depend on • Local extent • Isolated suture line recurrence after LAR • APR + Chemo/RT if no prior RT • Local recurrence without prior RT • PreOp chemo/RT, Surgery + IORT • Poor long-term DFS even with complete resection • Symptoms • Distant mets • Prior adjuvant therapy
CEA • 43-89% Sensitivity, 70-90% specificity • PreOp elevation predicts worse prognosis • Not useful in determining the need for adjuvant • Elevation correlates with Dukes’ stage • Persistent 1-month postOp elevation predicts mets • Monitor CEA q2-3 moths during chemo • Modest elevation • Fatty liver infiltration, hepatitis, pneumonia, GE
5-FU • 5 days IVP regimen: • Mucositis, diarrhea, neutropenia • Wkly IVP regimen: • Diarrhea • CI regimen/Capecitabine: • Hand-foot syndrome, mucositis • Diarrhea or neutropenia • High dose regimen 24-48hrs • Altered MS, angina-like chest pain
Oxaliplatin = Irinotecan • FOLFOX • FOLFIRI • XELOX • XELIRI • AVASTIN/ZALTRAP • ERBITUX/VECTIBIX • REGORAFENIB
Regional Therapy(Liver Mets) • HAI of FUDR via an implanted pump • Addition of dexamthazone reduces sclerosing cholangitis and enhances RR • Chemoembolization • 3mg/ml Adria + 3mg/ml MC + 10mg/ml CDDP with bovine collagen • Postembolization syndrome (fever, RtUQ pain, N/V, lethargy, hematologic toxicity) • Resection