Download
1 / 52
520 likes | 771 Views
Clinical Therapeutics in Obstetrics. Pregnancy and Prescription Medication Use: Quantifying Maternal, Placental and Fetal Pharmacology. Donald R Mattison Eunice Kennedy Shriver National Institute of Child Health and Human Development, NIH Donald.Mattison@nih.hhs.gov.

E N D
Clinical Therapeutics in Obstetrics Pregnancy and Prescription Medication Use: Quantifying Maternal, Placental and Fetal Pharmacology Donald R Mattison Eunice Kennedy Shriver National Institute of Child Health and Human Development, NIH Donald.Mattison@nih.hhs.gov
Clinical Therapeutics in Obstetrics • Introduction • Challenges for mechanistic models in pregnancy • Sex differences in pharmacokinetics and pharmacodynamics • Dynamics of maternal organism adapting to pregnancy • Dynamics of growth and development of the placenta • Dynamics of growth and development of the fetus • Improve precision and decrease uncertainty in predicting dose-exposure-response • Balance detail with utility 2
Clinical Therapeutics in Obstetrics • Three concerns for obstetrical clinical therapeutics • Dosing • Achieving “therapeutic concentrations” at the target site(s) • Efficacy/Effectiveness • Does the “therapeutic concentration” produce the desired effect(s) • Safety • What are the adverse consequences of exposure below, at, or above the “therapeutic concentration” • Biologically relevant models • Study design • Concentration and response at various target sites • Mother, Placenta or Fetus
Considerations for clinical therapeutics: Do pk and pd change during pregnancy? Role of the placenta: Drug metabolism, Transport, Target • Formal drug development process • Drugs used in pregnancy are developed informally, • migrating into use for: • Maternal disease • Fetal disease • Placental dysfunction 4
Drugs in development • Search of the PhRMA database of new medicines in development in the US (03 January 2011) • Hypertension in pregnancy: none • Preeclampsia: none • Gestational diabetes: none • Uterine hemorrhage: none • Labor pain: none • Obstetric and gynecological infection: none • Preterm labor: five • Labor disorders: none • Morning sickness: one • Neonatal infection: none • Neonatal jaundice: none • Respiratory distress syndrome: one • EMEA?
Clinical Therapeutics in Obstetrics • Introduction • Challenges for mechanistic models in pregnancy • Sex differences in pharmacokinetics and pharmacodynamics • Dynamics of maternal organism adapting to pregnancy • Dynamics of growth and development of the placenta • Dynamics of growth and development of the fetus • Improve precision and decrease uncertainty in predicting dose-response • Balance detail with utility 6
Clinical Therapeutics in Obstetrics • Introduction • Challenges for mechanistic models in pregnancy • Sex differences in pharmacokinetics and pharmacodynamics • Dynamics of maternal organism adapting to pregnancy • Dynamics of growth and development of the placenta • Dynamics of growth and development of the fetus • Improve precision and decrease uncertainty in predicting dose-response • Balance detail with utility 7
Hematological Changes During Pregnancy Gabbe et al 2007
Cardiovascular Changes During Pregnancy Gabbe et al 2007
Placental Changes During Pregnancy Surface area Increases from 3.2 m2 at 28 weeks to 12.6 m2 at term Distance between maternal and fetal blood Decreases from 50 – 100 u at 2nd month to 4 – 5 u at term Blood Flow Increases from 50 ml/min at 10 weeks to 600 ml/min at term 13 13
Translating Fetal Developmental Time from Experimental Species To Humans • Allometric relationships • Proportion of gestation • Proportion of development • Robinson & Dreher 1990 • Comparison of anatomical stages • Carnegie stages,Bayer et al. 1993 • Vulnerability patterns • Dobbing & colleagues 1970’s
Translating Fetal Neurodevelopmental Stages Across Species • Neurodevelopmental Stages • Sequence of neurodevelopmentalevents is conserved • Completion of neurodevelopmentalevents prior to birth varies acrossspecies • Timing of conception, birth and neurodevelopment species specific • Other tissues, organs, biologicalfunctions may also vary • Biological accuracy greatest uncertainty Clancy et al 2001
Clinical Therapeutics in Obstetrics • Introduction • Challenges for mechanistic models in pregnancy • Sex differences in pharmacokinetics and pharmacodynamics • Dynamics of maternal organism adapting to pregnancy • Dynamics of growth and development of the placenta • Dynamics of growth and development of the fetus • Improve precision and decrease uncertainty in predicting dose-response • Balance detail with utility 18
Model Parameters • Parent Compound and one metabolite • Maternal – 27 compartments • Fetal – 16 compartments • Physiologically complete • Biologically incomplete • Dynamic with respect to: • Maternal organism • Placenta • Fetus Luecke et al 1994
Maternal PB/PK Model (Placenta and Fetus) Gaohua et al 2010
General PB/PK Models Used in Pregnancy Corley et al 2003
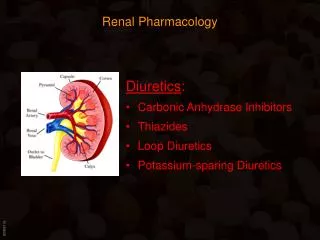
Glucose Transport Gude et al 2004 Schneider et al 2003 Illsley 2000
Saquinavir + P-gp inhibitors Saquinavir Molsa et al 2005
Caffeine Disposition in Pregnancy: Simcyp • Simulation parameters • Non-pregnant • 36 Weeks gestation • 150 mg caffeine • Pregnancy changescardiovascular, adipose,renal, metabolic, etc • Pregnancy compartment:placenta, fetus, amnioticfluid, mammary Gaohua et al 2010
Caffeine Water soluble - Vd ↑, [ ]↓ Metabolized by CYP1A2, XO, NAT Overall clearance ↓ during pregnancy Weeks Clearance 11 100% 17 68% 24 54% 32 37% PP 100%
Assessment of CYP1A2 Activity • Apparent oral clearance of caffeinedecreased during pregnancy • Suggesting CYP1A2 activity decreased during pregnancy (Tracy et al 2005)
Physiological accuracyis generally easier thanbiological accuracy Adding biologically andphysiologically relevantinformation enhances predictions Gaohua et al 2010
Case Examples:Treating the MomTreating the PlacentaTreating the Fetus
Influenza during pregnancy:Treating the Mom • Increased morbidity and mortality from influenza during pregnancy • Oseltamivr recommended medication at doses used in adults • No data on pharmacokinetics or pharmacodynamics in pregnancy • Dosing, efficacy and safety not described • Design a study to define how to effectively treat the mother
Oseltamivir • Pro-drug • Metabolized by carboxylesterases to active drug oseltamivir carboxylate (OC) • Disposition • Absorption • Substrate for GI PEPT1 • Active drug • Formed by hepatic carboxylesterase 1 • Distribution • Oseltamivir ~40% protein bound, OC ~5% • Oseltamivir substrate for P-gp • Very little access to fetal circulation • Placental perfusion studies • OC substrate for OAT3 (Slc22a8), MRP4 (Abcc4) • Elimination • Glomerular filtration • Tubular secretion • Blocked by probenecid
Prophylaxis Treatment
Early Data: Oseltamivir Carboxylate Beigi, R. H.; Han, K.; Venkataramanan, R.; Hankins, G. D.; Clark, S.; Hebert, M. F.; Easterling, T.; Zajicek, A.; Ren, Z.; Mattison, D. R.; Caritis, S. N., Pharmacokinetics of oseltamivir among pregnant and nonpregnant women. Am J Obstet Gynecol 2011.
Use of NSAIDS in pregnancy • Use of NSAIDS is common • Use in pregnancy carries fetal and neonatal risk • Constriction of ductus arteriosis • Persistant pulmonary hypertension • Use of human placental perfusion data for risk assessment and clinical support • Antipyrene • Salicylic acid • Diclofenac (monocarboxylate transporter) • Shintaku et al 2007, 2009, 2011 37
38 • Shintaku et al 2007, 2009, 2011
Relative Risk for DA Constriction: • Diclofenac > Salicylic Acid, Antipyrine • Case reports of DA Constriction: • Diclofenac > Salicylic Acid, Antipyrine • Shintaku et al 2007, 2009, 2011 39
Case Examples:Treating the MomTreating the PlacentaTreating the Fetus
Malaria: Treating the Placenta • Adverse impact • Pregnancy 2nd high-risk group after children • Maternal • Placental • Fetal • Therapy/prevention • Little data on dosing, efficacy, safety • “The kinetics, safety, and efficacy of available antimalarial drugs are poorly documented because pregnant women are systematically excluded from clinical trials” • Nosten, McGready and Mutabingwa Lancet Infectious Diseases 2007 • Failure of therapy high during pregnancy • Clear blood but after stopping treatment the infection re-emerges (genetic analysis)
Malaria in Pregnancy Placental infection • Placental Infection • Protected site • p falciparium • Necrosis • Growth restriction Desai et al 2007
Case Examples:Treating the MomTreating the PlacentaTreating the Fetus
Digoxin Toxicity Digoxin used to treat heart disease for >200 yrs High rate of toxicity Up to 30% if not carefully monitored Among those with digoxin toxicity 47% had life-threatening arrythmia 41% mortality Therapeutic monitoring Aarnoudse et al (2007) conducted a prospective population based study Women at ~2x greater risk than men Not known if pregnancy alters risk
Clinical Therapeutics in Pregnancy:Clinical Trials • Pregnancy does not diminish decision making capacity • Institute of Medicine (1994) • “…pregnant women be presumed eligible for participation in clinical studies” • Many IRBs and investigators consider pregnancy or reproductive age – exclusion criteria • Others suggest that exclusion is unethical • Dosing, efficacy, safety? • Only concern about clinical therapeutics during pregnancy is fetal safety
Inclusion in Clinical Trials • Declaration of Helsinki • No mention of research in pregnancy • 2002 Ethical Guidelines for Biomedical Research Involving Human Subjects • Guideline 17 • Pregnant women should be presumed eligible • UNAIDS/WHO ethical guidelines • …women throughout the lifespan…pregnant or breastfeeding…recipients of safe and effective interventions • How are “safe and effective interventions” identified? • Exclusion of women from research will deny them any benefit from the research