Download
1 / 35
1.01k likes | 3.72k Views
Renal Pharmacology. Diuretics : Carbonic Anhydrase Inhibitors Thiazides Loop Diuretics Potassium-sparing Diuretics. Renal Pharmacology. Kidneys : Represent 0.5% of total body weight, but receive ~25% of the total arterial blood pumped by the heart

E N D
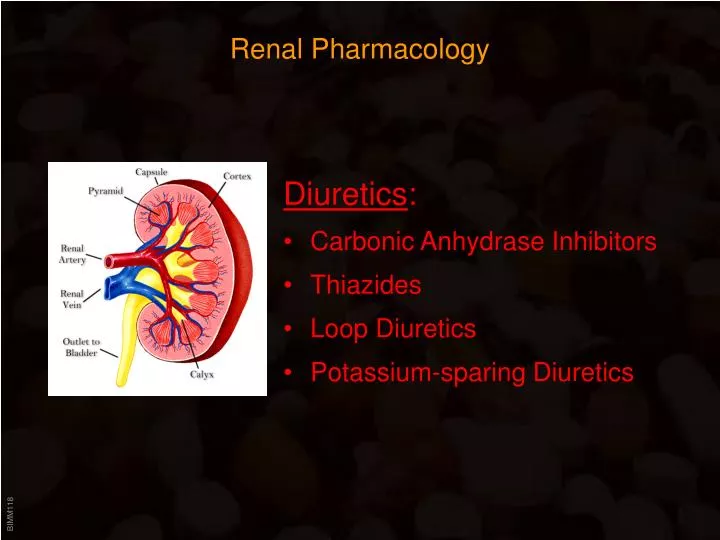
Renal Pharmacology Diuretics: • Carbonic Anhydrase Inhibitors • Thiazides • Loop Diuretics • Potassium-sparing Diuretics
Renal Pharmacology Kidneys: • Represent 0.5% of total body weight, but receive ~25% of the total arterial blood pumped by the heart • Each contains from one to two million nephrons: • The glomerulus • The proximal convoluted tubule • The loop of Henle • The distal convoluted tubule
Renal Pharmacology Functions • Clean extracellular fluid and maintain ECF volume and composition • Acid-base balance • Excretion of wastes and toxic substances • Renal processes • Filtration - glomerulus • Reabsorption • Tubular secretion In 24 hours the kidneys reclaim: • ~ 1,300 g of NaCl • ~ 400 g NaHCO3 • ~ 180 g glucose • almost all of the 180 L of water that entered the tubules
Renal Pharmacology • Blood enters the glomerulus under pressure • This causes water, small molecules (but not macromolecules like proteins) and ions to filter through the capillary walls into the Bowman's capsule • This fluid is called nephric filtrate • Not much different from interstitial fluid • Nephric filtrate collects within the Bowman's capsule and flows into the proximal tubule: • Here all of the glucose and amino acids, >90% of the uric acid, and ~60% of inorganic salts are reabsorbed by active transport • The active transport of Na+ out of the proximal tubule is controlled by angiotensin II. • The active transport of phosphate (PO4)3- is regulated (suppressed by) the parathyroid hormone. • As these solutes are removed from the nephric filtrate, a large volume of the water follows them by osmosis: • 80–85% of the 180 liters deposited in the Bowman's capsules in 24 hours • As the fluid flows into the descending segment of the loop of Henle, water continues to leave by osmosis because the interstitial fluid is very hypertonic: • This is caused by the active transport of Na+ out of the tubular fluid as it moves up the ascending segment of the loop of Henle • In the distal tubules, more sodium is reclaimed by active transport, and still more water follows by osmosis.
Renal Pharmacology Diuretics: • Increase output of urine • Primary indications are hypertension and mobilization of edematous fluid (e.g. kidney problems, heart failure, cirrhosis,…) Basic mechanism: • Block reabsorption of sodium and chloride => water will also stay in the nephron • Diuretics that work on the earlier nephron have greatest effect, since they are able to block more sodium and chloride reabsorption
Renal Pharmacology Diuretics: Carbonic anhydrase inhibitors: • Azetazolamide • Can trigger metabolic acidosis • Not in use as diuretic anymore • Primary indications is glaucoma (prevents production of aequous humor) • Dorzolamide CA-inhibitors are sulfonamides =>cross-allergenic with antibiotics etc.
Renal Pharmacology Diuretics: Loop diuretics (= high ceiling diuretics): • Strong, but brief diuresis (within 1 hr, lasts ~ 4hrs) • Used for moderate to severe fluid retention and hypertension • Most potent diuretics available • Act by inhibiting the Na+/K+/2Cl- symporter in the ascending limb in the loop of Henle • Major side effects: loss of K+ (and Ca++ and Mg++) • Furosemide • Bumetanide • Torasemide
Renal Pharmacology Diuretics: Thiazide diuretics: • Used for mild to moderate hypertension, mild heart failure, • Most potent diuretics available • Act by inhibiting the Na+/Cl- symporter in the distal convoluted tube • Major side effects: loss of K+ (and Mg++, but not Ca++) • Hydrochlorothiazide • Benzthiazide • Cyclothiazide …
Renal Pharmacology Major side effects of these diuretics: • Hypokalemia, hyponatremia, hypochloremia • Hypotension and dehydration • Interaction with Cardiac Glycosides => Potassium can be given orally or IV or Potassium-sparing diuretics: • Often used in combination with high-ceiling diuretics or thiazides due to potassium-sparing effects • Produce little diuresis on their own
Renal Pharmacology Diuretics: Potassium-sparing diuretics: • Act on the distal portion of the distal tube (where Na+ is exchanged for K+) • Aldosterone promotes reabsorption of Na+ in exchange for K+ (transcriptionally upregulates the Na+/K+ pump and sodium channels) • Spironolactone • Aldosterone receptor antagonist • Onset of action requires several days • Amiloride; Trimterene • Block sodium channels • Quick onset Aldosterone
Renal Pharmacology Diuretics: Potassium-sparing diuretics: • Act on the distal portion of the distal tube (where Na+ is exchanged for K+) • Aldosterone promotes reabsorption of Na+ in exchange for K+(transcriptionally upregulates the Na+/K+ pump and sodium channels) • Spironolactone • Aldosterone receptor antagonist • Onset of action requires several days • Amiloride; Trimterene • Block sodium channels • Quick onset Aldosterone Spironolactone
Renal Pharmacology Diuretics: Osmotic diuretics: • Small, non-reabsorbable molecules that inhibit passive reabsorption of water • Predominantly increase water excretion without significantly increasing Na+ excretion => limited use • Used to prevent renal failure, reduction of intracranial pressure(does not cross blood-brain barrier => water is pulled out of the brain into the blood) • Mannitol • Only given IV – can crystallize (=> given with filter needle or in-line filter)
Renal Pharmacology Uric acid • only slightly soluble in water and easily precipitates out of solution forming needle-like crystals of sodium urate • sodium urate crystals contribute to the formation of kidney stones and • produce the excruciating pain of gout when deposited in the joints. • Curiously, our kidneys reclaim most of the uric acid filtered at the glomeruli. Why, if it can cause problems? • Uric acid is a potent antioxidant and thus can protect cells from damage by reactive oxygen species (ROS). • The concentration of uric acid is 100-times greater in the cytosol than in the extracellular fluid. So when lethally-damaged cells release their contents, crystals of uric acid form in the vicinity. These enhance the ability of nearby dendritic cells to "present" any antigens released at the same time to T cells leading to a stronger immune response. => risk of kidney stones and gout may be the price we pay for these protections. • Most mammals have an enzyme — uricase — for breaking down uric acid into a soluble product. However, during the evolution of great apes and humans, the gene encoding uricase became inactive. • Uric acid is the chief nitrogenous waste of insects, lizards, snakes and birds (the whitish material that birds leave on statues)
Renal Pharmacology Uricosuric agents: • At therapeutic doses promote excretion and inhibit reabsorption of uric acid (normally, only 8-12% of the initially filtered urates are eliminated) • At low, subtherapeutic doses, both excretion and reabsorption are inhibited => possibility of an increase in uric acid concentration • Probenicid • Inhibits reabsorption of urates in the proximal convoluted tubule • Strong inhibitory effect on penicillin excretion • Sulfinpyrazone
Gastrointestinal Pharmacology • Antacids • Peptic ulcer therapy • Antiemetics • Laxatives • Antidiarrheal drugs
Gastrointestinal Pharmacology Acid production: • 2.5 L per day • Isotonic HCl solution • pH < 1 • Produced by parietal cells Mucus production: • Produced by mucus-secreting cells • Also produce bicarbonate, which becomes trapped in the mucus layer => pH gradient across the mucus layer (can become destroyed by alcohol)
Gastrointestinal Pharmacology Antacids: Weak bases: • Aluminum hydroxide • Cause constipation • Magnesium hydroxide • Cause diarrhea => often combined Usally taken 5-7 times per day
Gastrointestinal Pharmacology Antacids: • Histamine stimulates acid production by parietal cells • Mast cells produce a steady basal level of histamine,which increases in response to gastrin or acetylcholine • Parietal cells express histamine H2 receptors => H2 receptor blockers: • Cimetidine (Tagamet®) • First H2-blocker available • Inhibits P450 => Drug interaction • Ranitidine (Zantac®) • Does not inhibit P450 => fewer side effects • Nizatidine (Axid®) • Famotidine (Pepcid®)
Gastrointestinal Pharmacology Antacids: Proton pump inhibitors: • Irreversibly inhibit the H+/K+ - ATPase in gastric parietal cells • Drugs are inactive at neutral pH, but since they are weak bases,are activated in the acidic stomach milieu => restricted activity • Acid production abliterated for 24-48 hours • Omeprazole (Prilosec®) • Lansoprazole (Prevacid®) • Esomeprazole (Nexium®) • Rabeprazole
Gastrointestinal Pharmacology Gastroesophageal reflux disease (GERD): • Backflowof stomach acid into the esophagus • Esophagus is not equipped to handle stomach acid => scaring • Usual symptom is heartburn, an uncomfortable burning sensation behind the breastbone (MI often mistaken for GERD !) • More severe symptoms: difficulty swallowing, chest pain • Reflux into the throat can cause sore throat • Complications include esophageal erosions, esophageal ulcer and narrowing of the esophagus (esophageal stricture) • In some patients, the normal esophageal lining or epithelium may be replaced with abnormal (Barrett's) epithelium. This condition (Barrett's esophagus) has been linked to cancer of the esophagus. • Primary treatment option are proton pump inhibitors
Gastrointestinal Pharmacology Mucosal protective agents: • Misoprostol • Prostaglandin E1 analog (PG stimulate mucus and bicarbonate production) • Used when treatment with NSAIDs inhibits endogenous PG synthesis • Sucralfate • Complex of aluminum hydroxide and sulfated sucrose • Forms complex gels with mucus => mucus stabilized => diffusion of H+ impaired • Not absorbed => essentially free of side effects • Must be taken every 6 hours
Gastrointestinal Pharmacology Peptic Ulcer Disease Imbalance between defenses and aggressive factors • Defensive factors: Prevent the stomach and duodenum from self-digestion • Mucus: continually secreted, protective effect • Bicarbonate: secreted from endothelial cells • Blood flow: good blood flow maintains mucosal integrity • Prostaglandins: stimulate secretion of bicarbonate and mucus, promote blood flow, suppress secretion of gastric acid • Aggressive factors: • Helicobacter pylori: gram negative bacteria, can live in stomach and duodenum, may breakdown mucus layer => inflammatory response to presence of the bacteria also produces urease – forms CO2 and ammonia which are toxic to mucosa • Gastric Acid: needs to be present for ulcer to form => activates pepsin and injures mucosa • Decreased blood flow: causes decrease in mucus production and bicarbonate synthesis, promote gastric acid secretion • NSAIDS: inhibit the production of prostaglandins • Smoking: nicotine stimulates gastric acid production
Gastrointestinal Pharmacology Peptic Ulcer Disease (~25 mill. Americans will have an ulcer in their life) Most common cause (> 85%):Helicobacter pylorii (not stress or hot sauce!) Treatment options: • Antibiotics • Antisecretory agents • Mucosal protectants • Antisecretory agents that enhance mucosal defenses • Antacids
Gastrointestinal Pharmacology Antibiotic ulcer therapy: Combinations must be used: • Bismuth (PeptoBismol®) – disrupts cell wall of H. pylori • Clarithromycin – inhibits protein synthesis • Amoxicillin – disrupts cell wall • Tetracyclin – inhibits protein synthesis • Metronidazole – used often due to bacterial resistance to amoxicillin and tetracyclin, or due to intolerance by the patient Standard treatment regimen for peptic ulcer: Omeprazole + amoxicillin + metronidazole
Gastrointestinal Pharmacology Antiemetic drugs: Vomiting: • Infection, pregnancy, motion sickness, adverse drug effects,… • Triggered by the “vomiting center” or “chemoreceptor trigger zone (CTZ)” in the medulla (CTZ is on the ‘blood side’ of the blood-brain barrier). Treatment options: • H1 antagonists: Meclizine, promethazine, dimenhydramine… • Muscarinic receptor antagonists: Scopolamine (motion sickness) • Benzodiazepines: Lorazepam (during chemotherapy) • D2 antagonists:have also peripheral prokinetic effects => increase motility of the GI tract => increases the rate of gastric emptying. Caution in patients with Parkinson’s disease! Metoclopramide Domperidone • Cannabinoids: Marihuana ? Synthetic cannabinoids: during chemotherapy Nabilone Dronabinol
Gastrointestinal Pharmacology Laxatives: • Laxative – production of a soft formed stool over a period of 1 or more days • Catharsis – prompt, fluid evacuation of the bowel, more intense Indications for laxative use: • Pain associated with bowel movements • To decrease amount of strain under certain conditions • Evacuate bowel prior to procedures or examinations • Remove poisons • To relieve constipation caused by pregnancy or drugs Contraindications: • Inflammatory bowel diseases • Acute surgical abdomen • Chronic use and abuse
Gastrointestinal Pharmacology Laxatives: • Stimulate peristalsis • Soften bowel contect Classification: • Bulk laxatives • Non-absorbable carbohydrates • Osmotically active laxatives • Irritant laxatives = purgatives • Small bowel irritants • Large bowel irritants • Lubricant laxatives • Paraffin • Glycerol
Gastrointestinal Pharmacology Laxatives: Bulk laxatives: Increase in bowel content volume triggers stretch receptors in the intestinal wall => causes reflex contraction (peristalsis) that propels the bowel content forward Carbohydrate-based laxatives • Insoluble and non-absorbable • Non digestable; take several days for effect • Expand upon taking up water in the bowel • Must be taken with lots of water • Vegetable fibers (e.g. Psyllium, lineseed) • Bran (husks = milling waste product) Osmotically active laxatives • Partially soluble, but not absorbable • Saline-based (mostly sulfates) • Effect in 1-3 hrs => used to purge intestine (e.g. surgery, poisoning) • MgSO4 (= Epsom salt) • Na2SO4 (= Glauber’s salt)
Gastrointestinal Pharmacology Laxatives: Irritant laxatives: Cause irriatation of the enteric mucose => more water is secreted than absorbed => softer bowel content and increased peristaltic due to increase volume Small bowel irritants • Ricinoleic acid (Castor oil) • Active ingredient of Ricinus communis • The oil (triglyceride) is inactive • Ricinoleic acid released from oil through lipase activity Ricin: • Lectin from the beans of R.communis • Potent toxin: inhibits protein synthesis • Potential bioterrorism agent (LD ~100mg) In 1978, ricin was used to assassinate Georgi Markov, a Bulgarian journalist who spoke out against the Bulgarian government. He was stabbed with the point of an umbrella while waiting at a bus stop near Waterloo Station in London. They found a perforated metallic pellet embedded in his leg that had presumably contained the ricin toxin.
Gastrointestinal Pharmacology Laxatives: Irritant laxatives: Large bowel irritants Anthraquinones Active ingredient of Senna sp. (Folia and fructus sennae), Rhamnus frangulae (cortex frangulae) and Rheum sp. (rhizoma rhei): contain inactive glycosides => active anthraquinones released in colon take 6-10 hours to act
Gastrointestinal Pharmacology Laxatives: Irritant laxatives: Large bowel irritants Diphenolmethanes • Derivatives of phenolphtalein • Bisacodyl • Oral administration: effect in 6-8 hrs • Rectal administration: effect in 1 hr • Often used to prepare for intestinal surgery • Sodium picosulfate
Gastrointestinal Pharmacology Laxative abuse: Most common cause of constipation! • Longer interval needed to refillcolon is misinterpreted asconstipation => repeated use • Enteral loss of water and salts causes release of aldosterone=> stimulates reabsorption inintestine, but increases renalexcretion of K+ => double loss ofK+ causes hypokalemia, whichin turn reduces peristalsis. This is then often misinterpreted asconstipation => repeated use
Gastrointestinal Pharmacology Antidiarrheal drugs: • Diarrhea is usually caused by infection, toxins, anxiety, drugs… • In healthy adults mostly discomfort and inconvenience • In children (particularly mal-nourished) a principal cause of deathdue to excessive loss of water and minerals. Antimotility agents: • Muscarinic receptor antagonsists (not useful due to side effects) and opiates: • Morphine • Codeine • Diphenoxylate • All have CNS effects - NOT useful for diarrhea treatment • Loperamide • Selective action on the GI tract • Does not produce CNS effects • First choice antidiarrheal opoid • Combined with Dimethicone (Silicon-based gas-absorbent)
Gastrointestinal Pharmacology Antidiarrheal drugs: treat only symptoms! • Diarrhea is usually caused by infection (Salmonella, shigella, campylobacter, clostridium, E. coli), toxins, anxiety, drugs… • In healthy adults mostly discomfort and inconvenience • In children (particularly mal-nourished) a principal cause of deathdue to excessive loss of water and minerals. Antimotility agents: • Muscarinic receptor antagonists (not useful due to side effects) and opiates: • Morphine • Codeine • Diphenoxylate • All have CNS effects - NOT useful for diarrhea treatment • Loperamide • Selective action on the GI tract • Does not produce CNS effects • First choice antidiarrheal opoid Adsorbents: • Pectin, charcoal, kaolin…