Download
1 / 17
170 likes | 358 Views
A divergent tale of two cities. Colin Brown BSc MSc ( Epi ) MBChB MRCP FRCPath. Why HIV control in men who have sex with men may have differed between London and San Francisco since 2006?.

E N D
A divergent tale of two cities Colin Brown BSc MSc (Epi) MBChB MRCP FRCPath Why HIV control in men who have sex with men may have differed between London and San Francisco since 2006? CS Brown1,2, M Das3,4, L Hsu4, I Hall5, A Brown1, A Aghaizu1, P Birrell1, N Carraher4, S Desai1, J Hecht6, G Hughes1, D Mercey7, A Nardone1, T Packer4, F Post2, A Zaman1, Z Yin1, N Gill1, V Delpech1 1 2 3 4 5 6 7
Acknowledgements • Sincere thanks to all colleagues who have generously contributed their time, expertise, and on occasion, unpublished data in London and San Francisco • All the men who participated in the various behavioural surveys
Background & Methods • HIV endemic in both settings • 24% prevalence SF (64,000 MSM); 9% London (234,000 MSM) • Similar total prevalent numbers diagnosed • 13,000 SF; 14,000 London (2010) • Recent treatment differences • ART initiation at any CD4 count SF; ≤350 cells/μLLondon • SF decline in the undiagnosed, new diagnoses & incidence estimates – London largely static • Extensive surveillance/behavioural data from 2004 • Evaluate how differences in risk behaviour, testing and treatment coverage may account for the divergent trends
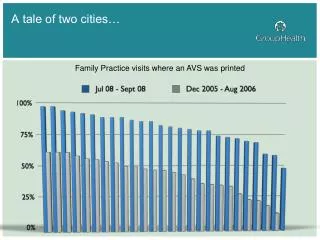
New diagnoses -increasing in London, decreasing in SF • * • Sources: SFDPH, PHE MPES, *Data as of Jan 2014
Incidence, undiagnosed and recency estimates – decreasing in SF London • Decrease in SF undiagnosed robust to sensitivity analysis: • Incidence estimates • New diagnoses • Inmigration estimates • Deaths SF • Sources: SFDPH, Phillips (PLoSOne, 2013) • Sources: NHBS, Birrell (Lancet ID, 2013), PHE MPES
Comparable MSM hubs – intensive interventions could be replicated • HIV Epidemiology London, 2011, HPA • HIV Report, 2011, SFDPH Castro Vauxhall
Median CD4 and age at diagnosis – similar across both settings R2 – 0.916 • Sources: CDC, PHE MPES
Testing patterns – more regular testing in SF Self-report Actual tests Sources: GUMCAD, SFDPH HIV Prevention Department Sources: Gay Men’s Sexual Health Survey, NHBS Higher frequency of self-reported testing Higher frequency of community sexual health tests Retest SF 6 months (28%); London 12 months (39%) Sources: Thorton, Magnet (unpublished)
Self-reported condomless sex – higher risk in London HIV negative MSM San Francisco:6m London:12m +ve (all UAI) +ve (all UAI) -ve (all UAI) -ve (all UAI) +ve (discordant) -ve(discordant) • Source: Gay Men’s Sexual Health Survey Year • Sources: STOP AIDS Project, NHBS
STIs largely concentrated in HIV positive MSM in SF • Sources: SFDPH STD, PHE GUMCAD
Care cascade differences Increasing retention in SF may allow for greater reduction in transmission London’s main problem is the static undiagnosed population • Sources: CDC & NHBS • Sources: PHE SOPHID/MPES
% MSM suppressed among diagnosed R2 – 0.970 • Sources: PHE SOPHID/MPES, CDC
Substance use and other markers of high risk – increasing in London • HCV reinfection rate up to 25% in 2 years in London SF HCV prevalence stable, likely older infections • Recreational drug use prevalent during London Shigellaflenerioutbreak • 76% recreational drug use • 31% injection drug use • London - 13.6% crystal meth use last year & 3.5% injection drug use (12% per year in SF, and decreasing) • Sources: Martin, AIDS, 2013; Gilbart, Lancet, 2014; • Bourne, SIGMA, 2014 ; Raymond, JAIDS, 2013
SF social marketing • Source: STOP AIDS • Source: STOP AIDS
Summary • Caveats - MSM denominator assumptions; comparable reporting mechanisms; shared population characteristics • Apparent reduced proportion of undiagnosed HIV and new diagnoses in SF may be due to: • Higher proportion of HIV-negative MSM reporting more regular HIV testing (and possible retesting) • Safer sex practices - increased condom use, disclosure, and seroadaptive practices • Culture of ‘positive’ openness • Critical importance for prevention of very high rates of HIV testing, awareness, and disclosure of HIV status • Safety myth of negative-negative serosorting needs aggressively challenged
Key next questions • How best to implement novel risk reduction strategies in London? • Achieving SF’s testing patterns/status disclosure challenging • Larger, less dense, lower prevalence population • Campaign methods: social media, community marketing, other? • Who is driving transmission in London vs SF? • Acute, undiagnosed or untreated infections • Contribution of inmigration (~20% new diagnoses in 2011) • Behaviour data needs disaggregated by: • Treatment uptake • Viraemia • PreP use
Selected data sources London San Francisco CDC HIV Surveillance data Consensus Meetings on HIV/AIDS Incidence and Prevalence in California National HIV Behavioural Surveillance Survey San Francisco AIDS Foundation SFDPH STD data SFPDH HIV Prevention data SFPDH HIV Epidemiology data STOP AIDS Project UCSF United States Census Bureau Literature review • Gay Men’s Sexual Health Survey (UCL) • Gay Men’s London Gym Survey • Gay Men’s Sex Survey (SIGMA) • National Survey of Sexual Attitudes and Lifestyles II • Office of National Statistics • PHE Genitourinary Medicine Clinic Activity Dataset (GUMCAD) • PHE HIV and AIDS New Diagnoses Database (HANDD) • PHE Multi-Parameter Evidence Synthesis (MPES) • PHE Recent Infection Testing Algorithm (RITA) • PHE Survey of Prevalent HIV Infections Diagnosed (SOPHID)