Download
1 / 1
10 likes | 118 Views
Contraception and Family Planning in HIV Prevention Trials: Current Practice and Stakeholder Perspectives Sean Philpott ¹ , ³ , Bridget Reutener Hanes ² , Katherine West Slevin¹, Monica Ruiz², Amita Vyas²

E N D
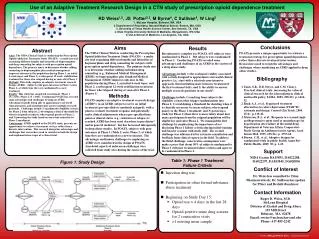
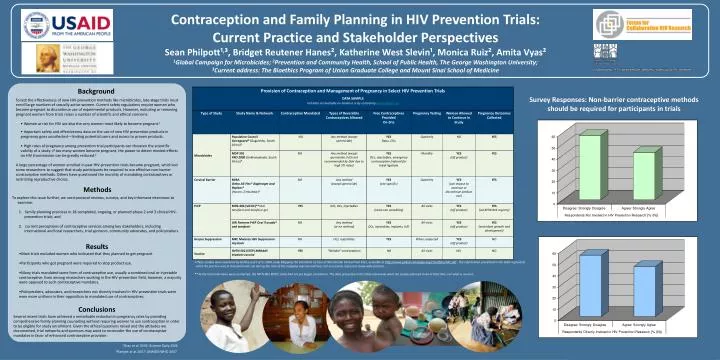
Contraception and Family Planning in HIV Prevention Trials: Current Practice and Stakeholder Perspectives Sean Philpott¹,³, Bridget Reutener Hanes², Katherine West Slevin¹, Monica Ruiz², Amita Vyas² 1Global Campaign for Microbicides; 2Prevention and Community Health, School of Public Health, The George Washington University; 3Current address: The Bioethics Program of Union Graduate College and Mount Sinai School of Medicine Background Survey Responses: Non-barrier contraceptive methods should be required for participants in trials • To test the effectiveness of new HIV-prevention methods like microbicides, late-stage trials must enroll large numbers of sexually active women. Current safety regulations require women who become pregnant to discontinue use of experimental products. However, excluding or removing pregnant women from trials raises a number of scientific and ethical concerns: • Women at risk for HIV are also the very women most likely to become pregnant.1 • Important safety and effectiveness data on the use of new HIV prevention products in pregnancy goes uncollected—limiting potential users and access to proven products. • High rates of pregnancy among prevention trial participants can threaten the scientific validity of a study: if too many women become pregnant, the power to detect modest effects on HIV transmission can be greatly reduced.2 • A large percentage of women enrolled in past HIV-prevention trials became pregnant, which led some researchers to suggest that study participants be required to use effective non-barrier contraceptive methods. Others have questioned the morality of mandating contraceptives or restricting reproductive choice. Methods • To explore this issue further, we used protocol reviews, surveys, and key informant interviews to examine: • family planning practices in 18 completed, ongoing, or planned phase 2 and 3 clinical HIV-prevention trials; and • current perceptions of contraceptive services among key stakeholders, including international and local researchers, trial sponsors, community advocates, and policymakers. Results • Most trials excluded women who indicated that they planned to get pregnant. • Participants who got pregnant were required to stop product use. • Many trials mandated some form of contraceptive use, usually a combined oral or injectable contraceptive. Even among researchers working in the HIV-prevention field, however, a majority were opposed to such contraceptive mandates. • Policymakers, advocates, and researchers not directly involved in HIV-prevention trials were even more uniform in their opposition to mandated use of contraceptives. • These studies were examined by GCM as part of its 2006 study Mapping the Standards of Care at Microbicide Clinical Trial Sites, available at http://www.global-campaign.org/clientfiles/SOC.pdf . The information presented in the table represents • what the practice was at that particular site during the time of the mapping exercise and does not necessarily represent study-wide practice.. • ** At the time interviews were conducted, the MTN-003 VOICE study had not yet begun enrollment. The data presented in the table represents what the studies planned to do at that time, not what is current. Conclusions Several recent trials have achieved a remarkable reduction in pregnancy rates by providing comprehensive family planning counseling without requiring women to use contraception in order to be eligible for study enrollment. Given the ethical questions raised and the attitudes we documented, trial networks and sponsors may want to reconsider the use of contraceptive mandates in favor of enhanced contraceptive provision. 1Gray et al. 2005; Science Daily 2008 2Ramjee et al. 2007; UNAIDS/WHO 2007.