Download
1 / 16
170 likes | 485 Views
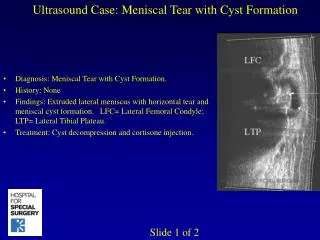
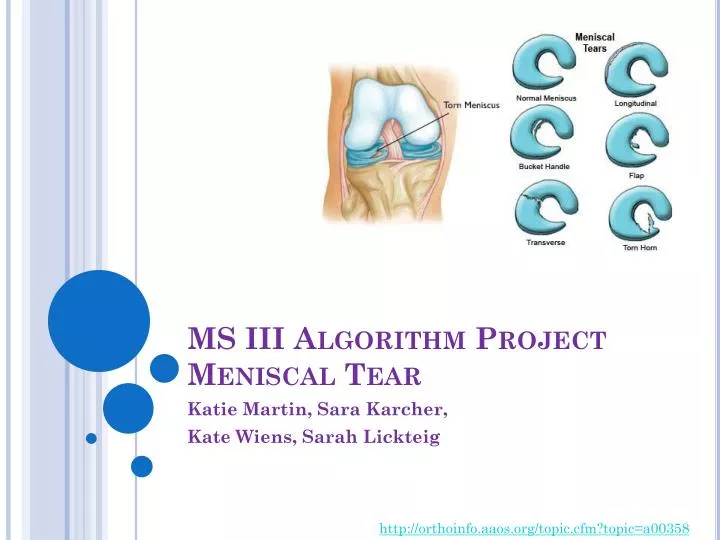
MS III Algorithm Project Meniscal Tear. Katie Martin, Sara Karcher , Kate Wiens , Sarah Lickteig. http://orthoinfo.aaos.org/topic.cfm?topic=a00358. Anatomy. Each knee contains a medial (c-shaped) and lateral (o-shaped) meniscus Made of fibrocartilage

E N D
MS III Algorithm ProjectMeniscal Tear Katie Martin, Sara Karcher, Kate Wiens, Sarah Lickteig http://orthoinfo.aaos.org/topic.cfm?topic=a00358
Anatomy • Each knee contains a medial (c-shaped) and lateral (o-shaped) meniscus • Made of fibrocartilage • Held in place by coronary ligaments externally and anchored by anterior and posterior “horns” internally • Transverse ligament connects the two menisci on the anterior tibia • Menisci sit on the articular surface of the tibia in order to seat the femoral condyles • Lateral meniscus moves freely, but the medial meniscus is more limited in motion, causing medial meniscus to be torn more often • Blood supply to the external border of the menisci is greater than to the innermost structure
Anatomy http://www.kneeandshouldersurgery.com/knee-disorders/meniscal-surgery.html http://images.yourdictionary.com/images/main/A4menisc.jpg
Biomechanics • Primary purposes of the menisci are to: • Protect tibiofemoral joint from compressive forces • Stabilize & guide joint movement • Lubricate the joint • Provide proprioception during flexion and extension and internal and external rotation of the tibiofemoral joint • The menisci follow the direction of the tibia during arthrokinematic movements: • Flexion tibia and menisci move posterior & into IR • Extension tibia and menisci move anterior & into ER relative to the femur
Mechanism of Injury • “Forceful, axial rotation of the femoral condyles over a partially flexed and weight-bearing knee” (Neumann 2010) • Medial meniscus may be injured when there is axial rotation coupled with a valgus force to the knee • There are many kinds of meniscal tears.
What Else Causes Knee Pain? • MCL Tear • LCL Tear • ACL Tear • PCL Tear • Osteoarthritis • Patellofemoral Bursitis • Patellofemoral Syndrome/Pain • OCD • Pes Anserine • ITBS • Plica Syndrome • RA • Bone Cancer • L3-S2 Irritation
Who is at Risk? • Most common in young athletes, especially if participating in sports that involve twisting and pivoting of the knee, like tennis, soccer, or basketball as well as contact sports like football • Peak age is 20-30 y/o (Loudon 2008) • Can also occur in older population (>40 y/o) due to degeneration of the cartilage • Overweight and obese people • Knee is misaligned or has history of ligamentous instability especially in the ACL • Conflicting evidence on males vs. females, but most resources said males have a greater risk than females with the ratio of 2.5 men to 1 female
Signs and Symptoms • A “pop” may be felt upon injury with gradual stiffness over the next 2-3 days • Joint line tenderness and possible effusion • Decreased knee ROM • Pt reports: “My knee hurts when I straighten it out” • Worsened symptoms by flexing and loading the joint • ex: squatting • Pain with turning, pivoting, twisting, going down stairs, getting up from a chair • C/o clicking, locking, catching, or giving way • Feelings of an unstable knee • Sharp pain with movement/dull ache at end of day • Gait abnormalities • 50% of acute injuries of ACL are associated with a concurrent injury to meniscus
Special Tests RULE IN: Meniscal Instability (medial or lateral) • McMurray’s Test: + test when clunk is felt/heard or reproductions of symptoms. • Apley’s Compression and Distraction Test: + test when clunk is felt/heard or reproduces symptoms (compression) and lessening of symptoms (distraction) • Grinds Test: + test when click or reproduction of symptoms • Thessaly: + test when sense of locking, catching and reproduction of symptoms • Ege’s Test: + test when reproduction of pain and or click is felt
Special Tests RULE OUT: Tibiofemoral Instability • Anterior Drawer Test: assesses integrity of ACL. + test when abnormal or excessive anterior translation of tibia as compared to other extremity • Lachman’s Test: assesses integrity of ACL. + test when abnormal or excessive anterior translation of tibia as compared to other extremity • Posterior Drawer Test: assesses integrity of PCL. + test when abnormal or excessive posterior translation of tibia as compared to other extremity • Posterior Sag: assesses integrity of PCL. + test when abnormal or excessive posterior translation of tibia as compared to other extremity • Valgus Stress Test (20-30 degrees): structures involved include MCL, PCL and posterior oblique ligament. + test when abnormal or excessive gapping compared to the other extremity • Varus Stress Test (20-30 degrees): structures involved include LCL, posteriolateral capsule, arcuate-popliteus complex, IT band, biceps femoris tendon. + test when abnormal or excessive gapping compared to the other extremity
Summary of Ranges for Sensitivity and Specificity of the Tests http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2796951/
Ege’s Test Internal Rotation External Rotation
Take Home Message How this algorithm will assist you in the clinic: • Follows exam sequence we learned • Includes Subjective and Objective Information • Clear and easy to follow • Literature supports the use of McMurray’s test, symptoms of giving-way and locking as best independent diagnostic tests of meniscal tear with 80% accuracy (Yan et al, 2011). • McMurray’s is best for diagnosing flap tear or radial tears in posterior lateral meniscus (Kim et al, 2012). • Special tests used to rule in have high specificity and tests used to rule out have high sensitivity • Added rule out tests to prevent biased results *Important to note that MRI is the gold standard for diagnostic imaging.
References • D Akseki, O Ozcan, H Boya, and H Pinar. A new weight-bearing meniscal test and a comparison with McMurray's test and joint line tenderness. Arthroscopy, The Journal of Arthroscopic & Related Surgery; Nov 2004; 20(9): 951-958 • Chivers, M. D., & Howitt, S. D. (2009). Anatomy and physical examination of the knee menisci: a narrative review of the orthopedic literature. The Journal of the Canadian Chiropractic Association, 53(4), 319-33. Retrieved from http://www.pubmedcentral.nih.gov/articlerender.fcgi?artid=2796951&tool=pmcentrez&rendertype=abstract • Dutton, M. (2004). Orthopaedic: Examination, evaluation, & intervention. New York, NY:McGraw-Hill. • Karachalios T, Hantes M, Zibis AH, Zachos V, Karantanas AH, Malizos KN. Diagnostic accuracy of a new clinical test (the Thessaly test) for early detection of meniscal tears. J Bone Joint Surg Am. 2005;87(5):955-962 • Kim, S., Hwang, B., Choi, D., & Mei, Y. (2012). The Paradoxial McMurray Test for the Detection of Meniscal Tears. The Journal of Bone and Joint Surgery. (94) e118. • Loudon, J., Swift, M., & Bell, S. (2008). The clinical orthopedic assessment guide. (2nd ed., pp. 307-308) • Milroy, D. (2012, February 13). The Human Knee, PTRS745. KUMC • Mohan, B. R., & Gosal, H. S. (2007). Reliability of clinical diagnosis in meniscal tears. International orthopaedics, 31(1), 57-60. doi:10.1007/s00264-006-0131-x • Neumann, D. A. (2010). Kinesiology of the Musculoskeletal System. (2nd ed.). St. Louis, MO: Mosby Elsevier. • Overweight patients face higher meniscal tear risk | Orthopedics. (n.d.). Retrieved April 22, 2013, from http://www.healio.com/orthopedics/knee/news/online/%7B9d61da87-2d5b-461b-850e-8ae95e5a6463%7D/overweight-patients-face-higher-meniscal-tear-risk • Urgery, S., Ncorporated, I., & Arthroscopic, A. (2012). The Paradoxical McMurray Test for the Detection of Meniscal Tears. Bone, 118(1), 1-7. • Yan, R., Wang, H., Yang, Z., Ji, Z. H., & Guo, Y. M. (2011). Predicted probability of meniscus tears: comparing history and physical examination with MRI. Swiss medical weekly, 141(December), w13314. doi:10.4414/smw.2011.1331 Retrieved from http://ptrs745.wikispaces.com/Knee on 4/22/13