Download
1 / 19
190 likes | 332 Views
State Fiscal Conditions and Medicaid. Robin Rudowitz Associate Director, Kaiser Commission on Medicaid and the Uninsured Henry J. Kaiser Family Foundation MAGNY Lunch March 16, 2012. Medicaid has m any r oles in o ur health care s ystem. Health Insurance Coverage

E N D
State Fiscal Conditions and Medicaid Robin Rudowitz Associate Director, Kaiser Commission on Medicaid and the Uninsured Henry J. Kaiser Family Foundation MAGNY Lunch March 16, 2012
Medicaid has many roles in our health care system. Health Insurance Coverage 29 million children & 15 million adults in low-income families; 15 million elderly and persons with disabilities Assistance to Medicare Beneficiaries 8.9 million aged and disabled — 21% of Medicare beneficiaries Long-Term Care Assistance 1 million nursing home residents; 2.8 million community-based residents MEDICAID Support for Health Care System and Safety-net 16% of national health spending; 40% of long-term care services State Capacity for Health Coverage Federal share can range from 50 - 83%; For FFY 2012, ranges from 50 - 74.2%
Medicaid eligibility levels are more limited for adults than for children. Median Medicaid/CHIP Eligibility Threshold January 2012 Minimum Medicaid Eligibility under Health Reform - 133% FPL ($24,645 for a family of 3 in 2011) SOURCE: Based on the results of a national survey conducted by the Kaiser Commission on Medicaid and the Uninsured and the Georgetown University Center for Children and Families, 2012.
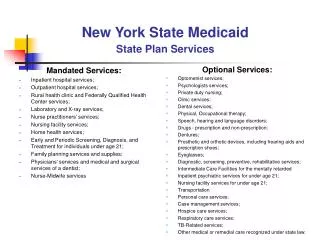
Most Medicaid enrollees receive care through private managed care. Comprehensive Medicaid Managed Care Penetrationby State, October 2010 ME VT WA NH MT ND MN OR MA NY WI SD ID MI RI CT WY PA NJ IA NE OH DE IN IL NV MD CO UT WV VA CA DC KS MO KY NC TN AZ SC OK AR NM GA AL MS LA TX AK FL HI 0% - 50% (9 states) 51% - 65% (15 states) U.S. Overall = 65.9% 66% - 80% (17 states and DC) 80%+ (9 states) NOTE: Includes enrollment in MCOs and PCCMs. Most data as of October 2010. SOURCE: KCMU/HMA Survey of Medicaid Managed Care, September 2011.
Medicaid provides access to care that is comparable to private insurance and better than access for the uninsured. 2010, PercentReporting: Adults Children Adults Children No Usual Source of Care Went Without Needed Care Due to Cost In past 12 months Questions about dental care were analyzed for children age 2-17. All other questions were analyzed for all children under age 18. MD contact includes other health professionals. Respondents who said usual source of care was the emergency room were included among those not having a usual source of care. All differences between the uninsured and the two insurance groups are statistically significant (p<0.05). SOURCE: KCMU analysis of 2010 NHIS data.
The elderly and disabled account for the majority of Medicaid spending. FY 2008, Total = 59.5 million FY 2008, Total = $317.7 billion NOTE: Percentages may not add up to 100 due to rounding. SOURCE:KCMU/Urban Institute estimates based on data from FY 2008 MSIS and CMS Form-64, 2010.
Medicaid enrollment and spending growth is accelerated during economic downturns. NOTE: Enrollment percentage changes from June to June of each year. Spending growth percentages in state fiscal year. SOURCE: Medicaid Enrollment June 2010 Data Snapshot, KCMU, February 2011. Spending Data from KCMU Analysis of CMS Form 64 Data for Historic Medicaid Growth Rates. FY 2011 and FY 2012 data based on KCMU survey of Medicaid officials in 50 states and DC conducted by Health Management Associates, September 2011.
Medicaid spending growth per enrollee has been slower than growth in private health spending. SOURCE: Urban Institute, 2010. Estimates based on data from Medicaid Financial Management Reports (HCFA/CMS Form 64), Medicaid Statistical Information System (MSIS), and KCMU/HMA enrollment data. Expenditures exclude prescription drug spending for dual eligibles to remove the effect of their transition to Medicare Part D in 2006.
Medicaid costs are shared by the states and the federal government. ME WA VT NH MT ND MN OR MA NY WI SD ID MI RI WY CT PA IA NJ NE OH DE IN IL NV MD CO UT WV VA CA DC KS MO KY NC TN AZ SC OK AR NM GA AL MS LA TX FL AK 50 percent (15 states) HI 51 – 59 percent (11 states) 60 – 66 percent (13 states) 67 – 74 percent (12 states including DC) NOTE: Rates are rounded to nearest percent. These rates will be in effect Oct. 1, 2011 – Sept. 30, 2012. SOURCE: Federal Register,, Nov, 10, 2010 (Vol. 75, No. 217), pp. 69082-69083. http://edocket.access.gpo.gov/2010/pdf/2010-28319.pdf
Medicaid is the second largest general fund budget item, but the largest source of federal funds for states. General Funds $619.1 B Federal Funds $552.7 B SOURCE: Actual FY 2010 data reported in: State Expenditure Report. NASBO, December 2011.
Shares of state General Fund spending for Medicaid and Educationhave remained fairly stable over time. Estimated SOURCE: NASBO Data from 2010 State Expenditure Report.
Medicaid helps to generate jobs in state economies. Federal Medicaid Matching Dollars — Injection of New Money State Medicaid Dollars Direct Effects Health Care Services Vendors (ex. Medical Supply Firm) Indirect Effects JOBS Employee Income Induced Effects Consumer Goods and Services Taxes
State Budget Gaps, SFYs 2002-2005 and 2009-2013 Measured in $Billions NOTE: This table describes aggregate state budget shortfalls or gaps between expected revenues and the amount needed to fund current services. Data represent shortfalls prior to actions to close the shortfalls and prior to accounting for offsets from ARRA. Figures are estimates for fiscal years 2011 and 2012 and projections for 2013. SOURCE: States Continue to Feel Recession's Impact. Center on Budget and Policy Priorities, February 2012.
Drops in revenues had a larger impact on state budgets than increases in Medicaid spending during the recession. Change in Annual State Revenues and Medicaid Spending, from SFY 2008 - SFY 2009, Measured in $Billions NOTES: Measure to determine drop in state revenues compared Total State Revenue (includes all sources of state revenues) in SFY 2009 to SFY 2008. Medicaid Spending comparison used total Medicaid spending (federal and state spending) that does not include administrative costs, accounting adjustments, or the U.S. Territories. SOURCES: 2008 and 2009 Annual Survey of State Government Finances. U.S. Census Bureau, 2011. KCMU and Urban Institute estimates based on data from HCFA/CMS (Form 64), 2010.
FY 2011 Adopted FY 2012 State Budget Pressures Result in Medicaid Cost Containment Efforts, But Eligibility is Protected NOTE: Past survey results indicate not all adopted actions are implemented. Provider payment restrictions include rate cuts for any provider or freezes for nursing facilities or hospitals. SOURCE: KCMU survey of Medicaid officials in 50 states and DC conducted by Health Management Associates, September 2011.
States with Provider Rate Changes FY 2009 – FY 2012 FY 2009 FY 2010 FY 2011 Adopted FY 2012 States with Rate Increases Inpatient Hospital Physicians MCOs Nursing Homes Any Provider States with Rate Restrictions NOTE: Past survey results indicate adopted actions are not always implemented. Any provider includes all other provider groups mentioned. Rate restrictions include rate cuts for any provider and also frozen rates for inpatient hospitals and nursing homes. SOURCE: KCMU survey of Medicaid officials in 50 states and DC conducted by Health Management Associates, September 2009, September 2010, and September 2011.
Expanding Medicaid is a key element in health reform. Universal Coverage Exchanges (subsidies 133-400% FPL) Medicaid Coverage (up to 133% FPL) Individual Mandate Health Insurance Market Reforms Employer-Sponsored Coverage NOTE: In 2009, 133% FPL for family of 4 is $29,327 and 400% FPL is $88,200
The federal government will pay for the vast majority of Medicaid coverage costs in health reform. Total $464.7 SOURCE: Analysis by the Urban Institute for the Kaiser Commission on Medicaid and the Uninsured. Medicaid Coverage and Spending in Health Reform: National and State-by-State Results for Adults at or Below 133% FPL. May 2010.
Looking Ahead • State Issues • States starting to see positive economic sign, but conditions vary across states • Focus remains on cost containment • Focus on delivery system reforms • Federal Issues • Federal deficit reduction efforts continue • Health reform • Supreme Court • Opportunities: Major reductions in the uninsured and uncompensated care, new opportunities for care coordination, focus on dual eligibles • Challenges: Timing, reduced state staffing levels, need for new eligibility and enrollment systems, concern about provider capacity