Download
1 / 22

E N D
ADHD By Rhian Uptegraft
What is AD/HD? • ADHD is a Disruptive Behavior Disorder characterized by the presence of a set of chronic and impairing behavior patterns that display abnormal levels of inattention, hyperactivity, or their combination. (According to the 1994, Diagnostic and Statistical Manual of Mental Disorders, Ed. IV,)
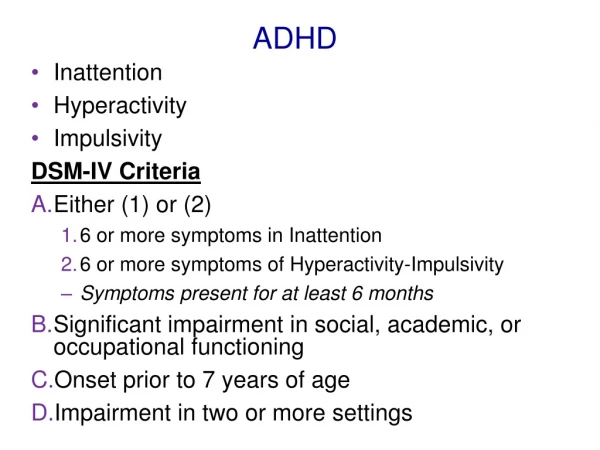
Characteristics & Facts • Symptoms -- AD/HD has 3 major subtypes • AD/HD - Primarily Inattentive Type:• Fails to give close attention to details or makes careless mistakes.• Has difficulty sustaining attention.• Does not appear to listen.• Struggles to follow through on instructions.• Has difficulty with organization.• Avoids or dislikes tasks requiring sustained mental effort.• Easily distracted.• Forgetful in daily activities.
AD/HD - Primarily Hyperactive/Impulsive Type: • Fidgets with hands or feet or squirms in chair.• Has difficulty remaining seated.• Runs around or climbs excessively.• Has difficulty engaging in activities quietly.• Acts as if driven by a motor.• Talks excessively.• Blurts out answers before questions have been completed.• Has difficulty waiting or taking turns.• Interrupts or intrudes upon others.
AD/HD - Combined Type: • Meets both inattentive and hyperactive/impulsive criteria. • Because everyone shows signs of these behaviors at one time or another, the guidelines for determining whether a child has AD/HD are very specific. • In children, the symptoms must be more frequent or severe than in other children of the same age. These behaviors must create significant difficulty in at least two areas of life, such as home, social settings and school.
Symptoms usually appear before the age of seven • This means all teachers must be prepared to encounter students with AD/HD. • Many students will enter kindergarten already carrying a diagnosis of AD/HD. • However, as teachers, we must also be prepared to recognize the symptoms of AD/HD in other students who have not been diagnosed, but are exhibiting them.
Diagnosis • There is not single test for diagnosing AD/HD. • It takes many steps by trained professionals to make a diagnosis of AD/HD. • The Diagnostic and Statistical Manual of Mental Disorders (DSM),published by the American Psychiatric Association, is the guide that lays out the criteria to be used by doctors, mental health professionals, and other qualified clinicians when making a diagnosis of AD/HD. • A good evaluation should first look to rule out other causes for the behavior of the child. • The evaluation should involve a clinical assessment of the child’s school, social and emotional functioning and developmental levels. • The child’s family and the teacher should maintain a detailed chronicle of the child’s daily activities. • If possible, it is good to have the child also track their own history. • It is the responsibility of the professionals to determine the diagnosis.
It is the most commonly diagnosed psychiatric disorder in children • It affects at least 3-5 percent of children in the world. • Roughly 4.5 million children in the U.S. (about 7 percent of that age group) have been diagnosed with AD/HD. • Breaking that number down shows that 11 percent of the boys in this age group have AD/HD, • while 4 percent of girls have been diagnosed with AD/HD. • That means boys are almost 3 times as likely to be diagnosed with AD/HD as are girls.
Attention-Deficit/Hyperactivity Disorder (AD/HD) is a neurobiological disorder • Neurobiological disorders are problems that affect the peripheral and central nervous systems of an individual. • The nervous system comprises the spinal cord, the brain, peripheral nerves, cranial nerves, the autonomic nervous system, nerve roots, muscles, and neuromuscular junction. • There are more than 600 neurological disorders ranging across a wide spectrum including Alzheimer's disease, epilepsy, migraines, Huntington's disease, muscular dystrophy and AD/HD that have been recognized. • Several areas of the brain may be affected by AD/HD according to modern research models describing what is happening in the brains of people with AD/HD.
The exact cause has not been determined • Unlike many diseases and disorders, there are no genetic markers, physical characteristics or simple test that can identify a child as having AD/HD. • Researchers have not identified the exact causes, but they are certain that heredity plays a major role. • When heredity can be ruled out, difficulties during pregnancy, prenatal exposure to alcohol and tobacco, premature delivery, significantly low birth weight, excessively high body lead levels, and postnatal injury to the prefrontal regions of the brain have all been found to contribute to the risk for AD/HD to varying degrees
AD/HD has been studied and documented for over 100 years • AD/HD is not a modern phenomenon. • It has surely been around longer than recorded history. • The key point is that it has gone through a curve of being recognized and defined that has included several name changes. • The first mention of a disorder that was surely AD/HD was in 1798. Sir Alexander Crichton describes "mental restlessness" in his book An Inquiry Into the Nature and Origin of Mental Derangement.
Treatment • Multimodal treatment is the most effective form of treatment for children and adolescents with AD/HD. • This treatment approach includes multiple elements which work best together and support each other. The elements of the multimodal treatment approach include: • Parent and child education about diagnosis and treatment • Specific behavior management techniques • Stimulant medication • Appropriate educational program and supports. • The level of response or non-response to any or all of these will be unique to each individual and cannot be predicted. • Working closely with health care providers and school personnel, treatment should be tailored to the unique needs of each child and family.
Behavioral Treatment • Psychosocial treatment is a critical part of treatment for AD/HD. • Behavior modification is the onlynonmedical treatment for AD/HD with a large scientific evidence base. • Behavior treatment involves both social and psychological therapies. • A detail article explain Behavioral Modification can be found at: http://www.help4adhd.org/en/treatment/behavioral/WWK7S
Misconceptions • Children outgrow AD/HD in adolescence • It was believed for a long time that people outgrow AD/HD as they mature. This is not true. • It is more common in boys than in girls • Boys are more than twice as likely to have AD/HD. However, some studies suggest that at least some of the difference is based in biases of the referring teachers. Do not assume that a child does not have AD/HD simply based on their gender.
Misconceptions • People with AD/HD cannot be successful as adults Not true! Look at these famous people: Vincent Van Gogh, Terry Bradshaw, Pete Rose, Mark Twain, Emily Dickenson, Ralph Waldo Emerson, Wolfgang Mozart, Andrew Carnegie, Henry Ford, Christopher Columbus, Ann Bancroft, Jim Carrey, Jack Nicholson, Elvis Presley, Justin Timberlake, Robin Williams, Thomas Edison, Benjamin Franklin, Alexander Graham Bell, Albert Einstein, John F. Kennedy, Abraham Lincoln.
Accommodations for individual students • Section 504 of the Rehabilitation Act of 1973 provides educational accommodations for students with ADHD who don't qualify for special education services. • That means we can all expect to encounter students with AD/HD during our tenure as teachers.
Lesson Plans and Instruction • Use visual aids. Put objectives on the blackboard • Try pair-share between students with 504 Plans and student peers in the classroom • Written outlines or lesson outcomes • Diversify learning modalities in the presentation of instructions and material • Incorporate technology in instruction • Divide lessons into smaller chunks of material • Employ a variety of assessments to verify understanding and mastery of learning objectives
Classroom Arrangement • Plan the seating to make learning more accessible. • Seat the students with 504 Plans with their student helpers whenever needed • Use proximity in lesson delivery • Reduce classroom distractions to help minimize overstimulation • Try group configurations with 4 students to a group
Assignment Modification • Provide extra time as needed for processing information and turning in assignments • Present smaller chunks of learning to aid in simplicity of outcome • Use a resource room to provide organizational and study skills • Do pre and post diagnostic assessments to validate learning materials • Allow students to use computer software to assist learning and writing assignments
Behavioral Cues • Provide the students feedback and appropriate celebrations • Encourage students to reflect and journal at the end or beginning of the class period • Give students proactive feedback when they engage in distracting behavior • Use non-verbal cues if possible for students if they need redirection • Post rules and consequences for the classroom. • Provide students with time-outs and teacher interaction when needed
Resources for additional information • www.chadd.org -- Children and Adults with Attention-Deficit/Hyperactivity Disorder (CHADD) • http://www.help4adhd.org – National Resource Center on AD/HD • http://www.nimh.nih.gov – National Institute of Mental Health • http://www.adhdsupport.com – AD/HD Support • http://add.about.com • http://www.help4adhd.org/index.cfm?varLang=en -- National Resource Center on AD/HD
Resources for additional information • http://en.wikipedia.org/wiki/AD/HD • http://www.cdc.gov/nchs/data/series/sr_10/Sr10_237.pdf -- CDC info, very detailed and informative. • http://www.napcse.org/exceptionalchildren/adhd/adhd-definition.php - The National Association of Parents with Children in Special Education