Download
1 / 120
1.2k likes | 1.4k Views
APPROPRIATE UTILIZATION OF BLOOD AND BLOOD COMPONENTS. Paul M. Ness, M.D. Director, Transfusion Medicine Johns Hopkins Medical Institutions Baltimore MD USA. 合理使用血液和血液成分. Paul M. Ness, M.D. 医学博士 约翰霍普金斯医学中心输血科主任 美国 - 马里兰州 - 巴尔的摩. MAJOR PATIENT CONCERNS.

E N D
APPROPRIATE UTILIZATION OFBLOOD AND BLOOD COMPONENTS Paul M. Ness, M.D. Director, Transfusion Medicine Johns Hopkins Medical Institutions Baltimore MD USA
合理使用血液和血液成分 Paul M. Ness, M.D.医学博士 约翰霍普金斯医学中心输血科主任 美国-马里兰州-巴尔的摩
MAJOR PATIENT CONCERNS • How safe are blood transfusions with respect to AIDS and other complications? • Are there any alternatives that I can use to avoid blood transfusions?
患者关注的主要内容 • 鉴于艾滋病和其他并发症,输血的安全性如何? • 是否有避免输血的替代治疗?
PERIOPERATIVE RED CELL TRANSFUSIONNIH CONFERENCE, 1988 • Transfusion trigger of 10 g/dl is NOT justified; 7 g/dl may be more appropriate. • Moderate perioperative anemia does not contribute to morbidity or delay wound healing. • Homologous transfusion should be minimized. • Alternatives to homologous transfusion should be encouraged.
围手术期红细胞输血美国国立卫生研究院大会, 1988年 • 血红蛋白10克/分升的输血指针还不充分, 7克/分升可能更为恰当 • 围手术期轻度贫血不会导致发病或延迟愈合 • 同种异体输血应减少到最低限度 • 应鼓励替代同种异体输血的方法
TRANSFUSION ALTERNATIVES • Predeposit autologous transfusion • Hemodilution • Intraoperative autologous transfusion • Pharmacologic therapies • Blood substitutes • Apheresis to reduce donor exposure • Pathogen inactivation
输血的替代方法 • 预存的自体血输注 • 血液稀释 • 术中的自体血输注 • 药物治疗 • 血液代用品 • 减少献血者暴露的机采 • 病原体灭活
血 液 成 分 全血 红细胞 富血小板血浆 血小板 新鲜冰冻血浆 血浆(成份分离) 冷沉淀 凝血因子
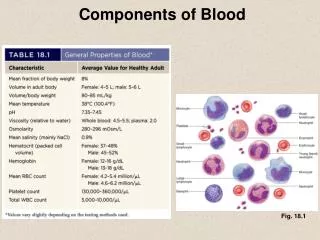
PREFERENTIAL USE OF COMPONENTS • Avoids circulatory overload • Limits harmful metabolic materials • Concentrates required material for effective levels • Minimizes risk of disease transmission • Maximizes use of donated blood
使用成分血的优点 • 避免循环超负荷 • 降低有害代谢物质 • 浓缩所需的成分至有效的水平 • 减少传染性疾病的危险 • 最大限度地利用捐献的血液
Red blood cells Leukocyte-depleted RBC Washed red cells Frozen red cells Reduce volume Remove leukocytes Remove plasma Increase storage period RED CELL COMPONENTS
红 细 胞 成 分 • 红细胞 • 去白红细胞 • 洗涤红细胞 • 冰冻红细胞 • 减少容量 • 去除白细胞 • 去除血浆 • 增加贮藏期
LEUKOCYTE DEPLETIONPOTENTIAL CLINICAL ADVANTAGES • Reduce transfusion reactions from WBC or cytokines • Reduce risk of alloimmunization • Reduce risk of infections from cell associated viruses (CMV) • Reduce risks of immunomodulation ( cancer recurrence, perioperative infections)
白细胞去除的潜在临床优势 • 减少白细胞或细胞因子引起的输血反应 • 降低同种异体免疫反应的风险 • 降低感染细胞相关病毒(巨细胞病毒)的风险 • 降低免疫调节的风险(癌症复发,围手术期感染)
Leukoreduction decreases mortality in cardiac surgery • Death rate reduced from 7.8% to 3.5% (van de Watering 1998), and 10.1% to 5.5% (Bilgin 2001) in randomized trials of leukoreduced transfusions • Post-operative infection has a mortality of 8-15% and is the leading cause of multiorgan failure syndromes N Blumberg MD & JM Heal MRCP
减 少 白 细 胞降低心脏外科手术的死亡率 • 在输注少白细胞血液的随机试验中,死亡率从7.8 %降到3.5 % ( van de Watering1998年) ,从10.1 %降到5.5 % ( Bilgin 2001 ) • 手术后感染的死亡率为8-15 % ,是导致多脏器衰竭综合症的主要原因
Number to treat to save one life(NTN) • Nucleic Acid Testing (NAT) for HIV/HCV 500,000 to 1,000,000 • Cost per life saved = $2.5-5,000,000 • Leukoreduction of allogeneic transfusions in cardiac surgery 20 • Cost per life saved = $400-600
(NNT)救治一人所需要的费用 • 艾滋病毒/丙型肝炎病毒的核酸检测(NAT) 500,000 到1,000,000 • 每个人的救治费用$2.5-5,000,000 • 心脏手术所用的减少白细胞的同种异体输血 20 • 每个人的救治费用$400-600
TRANSFUSION TRIGGERRed Blood Cells • Cardiac output increases with anemia, when hemoglobin falls below 7 grams/dl • Oxygen extraction increases with anemia • Lactic acidosis indicates failure of oxygen delivery; not useful as transfusion trigger • Normal animals develop cardiac failure at Hct of 10%; animals with coronary stenosis have heart failure at higher Hct (17%)
红细胞的输血指针 • 血红蛋白低于7克/分升时,导致心输出量增加和贫血 • 氧摄取增加和贫血 • 乳酸性酸中毒表明氧输送障碍;不能作为输血的指针 • 正常动物的红细胞压积在10 %时发生心力衰竭;伴冠状动脉狭窄的动物在较高红细胞压积(17 %)时发生心力衰竭
Is Anemia Harmful in the ICU? • Hebert et al (NEJM1999) compared a liberal transfusion strategy to a conservative regimen • 838 patients randomized to transfused hemoglobin levels of 7-9 g/dl or 10-12 g/dl • Morbidity and mortality was lower in patients with conservative regimen unless patients had unstable angina or MI.
贫血在重症监护病房是有害的吗? • 1999年Hebert等人在新英格兰医学杂志上将自由输血的策略与保守的治疗方案进行了比较。 • 838例输血患者按血红蛋白7-9克/分升或10-12克/分升的水平随机分组 • 除了不稳定型心绞痛或急性心肌梗死的患者,保守疗法患者的发病率和死亡率较低。
RBC transfusion “trigger” Primary outcome: 30 day mortality from all causes 18.7 23.3% Hebert, 1999
红细胞输血“指针” 主要结果:所有输血原因的30天死亡率分析 限制输血策略 18.7 自由输血策略 23.3%
Intraoperative Red Cell TransfusionAnesthesiologist Task Force, 1996 • Transfusion is rarely indicated when hgb > 10 and is almost always indicated when hgb< 6, especially with acute anemia • Transfusions for hemoglobin 6-10 g/dL should be based upon risk of complications of inadequate oxygenation. • Single hemoglobin trigger for all patients is not recommended • Use of autologous options or measures to reduce blood loss may be benefical • Trigger for autologous blood may be more liberal than for allogeneic red cells because of lower risks
术中红细胞输血,麻醉师工作组, 1996年 • 当血红蛋白> 10,很少需要输血;当血红蛋白< 6,特别是伴急性贫血时,几乎都需要输血。 • 血红蛋白6-10克/升的输血应考虑缺氧并发症的风险。 • 适用于所有患者的单一血红蛋白指针尚未提出 • 使用自体输血或减少失血的措施是有益的 • 因为低风险,自体输血的指针比输注异体红细胞更自由。
Inadequate Tx Therapy in WAIHA(Extracted from Plaintiff Law Suits)
温抗体型自身免疫性溶血性贫血中不充分的输血治疗(摘自原告诉讼)温抗体型自身免疫性溶血性贫血中不充分的输血治疗(摘自原告诉讼)
TRANSFUSION TRIGGERChronic Anemia • Cardiac output increases with anemia, when hemoglobin falls below 7 grams/dl • Oxygen extraction increases with anemia • Lactic acidosis indicates failure of oxygen delivery; not useful as transfusion trigger • Normal animals develop cardiac failure at 10% Hct; animals with coronary stenosis have heart failure at higher Hct (17%)
输血指针:慢性贫血 血红蛋白低于7克/分升时,导致心输出量增加和贫血 导致氧摄取增加和贫血 乳酸性酸中毒表明氧输送障碍;不能作为输血的指针 正常动物红细胞压积在10 %时发生心力衰竭;伴冠状动脉狭窄的动物在较高红细胞压积(17 %)时发生心力衰竭
Transfusion TriggerSevere Warm AIHA Maintain hemoglobin above 4 g/dL in younger patients, who often tolerate severe anemia if it has developed slowly For older patients or patients with known cardiovascular disease, maintain hemoglobin above 6 g/dL
输 血 指 针重度温抗体型自身免疫性溶血性贫血 • 如果是较年轻的患者,由于贫血发展缓慢,患者已耐受严重贫血,则应维持其血红蛋白在4克/分升以上。 • 对于年老或有心血管疾病患者,维持血红蛋白在6克/分升以上。
RED CELL INDICATIONS • Treatment of anemia in cases too severe to be treated by nutritional replacement or iron • Surgical blood loss greater than 10 - 15% of estimated blood volume • Correction of perioperative anemia to a hematocrit of approximately 25% • Hypotension associated with bleeding
红 细 胞 的 适 应 症 如果经营养支持或补铁治疗贫血仍严重,应输红细胞纠正贫血。 手术失血量大于总血量的10 -15% 纠正围手术期贫血使红细胞压积至25 % 低血压伴出血
Platelet Components Produced -- from whole blood platelet-rich plasma (PRP) buffy coat (in Europe) -- Platelet apheresis
血 小 板 成 分 从全血中制备 • 富血小板血浆 • 白膜法(欧洲) • 机采血小板
Pooled concentrates Lower costReadily available supply Apheresis Lower donor exposureLower reaction rate Limited donor pool PLATELET TRANSFUSIONS
血 小 板 输 血 汇集浓缩 价格低 已有效供应 机采 献血者低暴露 低反应率 最小程度的供者汇集
APHERESIS PLATELETSPOTENTIAL ADVANTAGES Reduction in infectious complications Reduction in transfusion reactions Ease of leukodepletion Reduction in transfusion frequency Treatment of alloimmunized recipients Prevention of alloimmunization (UNPROVEN) Platelet quality
机采血小板潜在的优点 • 减少感染并发症 • 减少输血反应 • 易于去白 • 减少输血频率 • 治疗同种异体免疫患者 • 预防同种异体免疫(未证实) • 血小板质量
INDICATIONS FOR PLATELET TRANSFUSIONS • Overt bleeding or prophylaxis • Most useful in clinical states of decreased platelet production • Less beneficial in states of increased • platelet destruction – DIC, ITP
血小板输血适应症 显性出血或预防性输注 多用于临床血小板产生减少的临床状态 血小板增生状态时则输注效果不明显 血小板破坏-弥漫性血管内凝血 ,特发性血小板减少性紫癫