Download
1 / 58
600 likes | 863 Views
MODULE 6. Bundle Branch Block and the Imitators of ACS. Bundle Branch Block. Can be pre-existing condition Can be caused by ACS. Bundle Branch Block. BBB caused by AMI 60%-70% association with pump failure 40%-60% mortality without reperfusion. Bundle Branch Block. Can mimic ACS

E N D
MODULE 6 Bundle Branch Block and the Imitators of ACS
Bundle Branch Block • Can be pre-existing condition • Can be caused by ACS
Bundle Branch Block • BBB caused by AMI • 60%-70% association with pump failure • 40%-60% mortality without reperfusion
Bundle Branch Block • Can mimic ACS • Can hide evidence of ACS
May Produce ST elevation ST depression Tall T waves Inverted T waves Wide Q waves May Hide ST elevation ST depression Tall T waves Inverted T waves Wide Q waves Bundle Branch Block
The Problem • Critical to reperfuse patients with BBB produced by ACS • ACS harder to identify on ECG when BBB present
The Solution • BBB Problem • New or presumably new BBB is an indication for fibrinolytic therapy
The Solution Fibrinolytic Therapy Trialists’ (FIT) Collaborative Group, 1994
BBB Recognition Forget About the Notch!
BBB Recognition • Wide QRS • > 120ms • Supraventricular rhythm
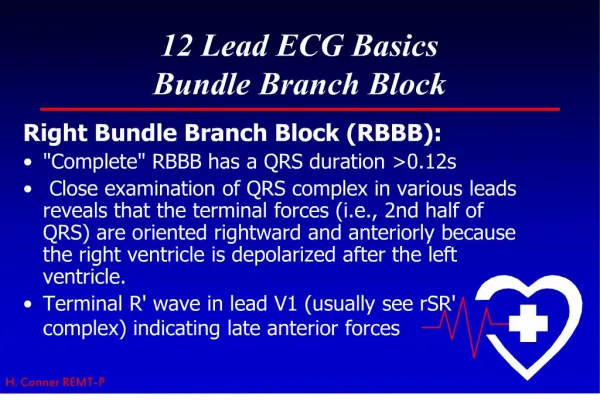
RBBB vs LBBB • RBBB in V1
RBBB vs. LBBB • LBBB in V1
RBBB vs. LBBB • Use V1 • Identify direction of terminal force
Bundle Branch Block • V1
BBB New onset BBB, or presumably new BBB, is an indication for acute reperfusion therapy
Ventricular Rhythms • Paced rhythms • Idioventricular rhythms • AIVR • V-Tach • PVC
Ventricular Rhythms • Can mask or mimic every ECG change suggestive of ACS
Left Ventricular Hypertrophy • Enlarged left ventricle • Pumping against increased resistance • Chronic overfilling
May Produce ST elevation ST depression Tall T waves Inverted T waves May Hide ST elevation ST depression Tall T waves Inverted T waves LVH
LVH • Does not abnormally widen QRS • Increases height and depth of QRS • Recognized by this increase • Three step recognition formula
LVH Recognition • Step 1 • Look in V1 and V2 • Pick the deepest negative deflection • Count small boxes of negative deflection in that lead • Remember that number
LVH Recognition • Step 2 • Look in V5 and V6 • Pick the tallest positive deflection • Count small boxes of positive deflection • Remember that number
LVH Recognition • Step 3 • Add the two numbers together • Suspect LVH if the sum equals 35 or more
Ventricular Aneurysm • NOT Aortic Aneurysm • “Bleb” in ventricle secondary to infarct • Bleb is dyskinetic • “Pops out” when ventricle contracts
Ventricular Aneurysm • Associated with persistent ST elevation • Often in V1-V4 • Can occur in any lead
Benign Early Repolarization • Normal variant • Produces • ST elevation • Tall T waves
Benign Early Repolarization • Changes usually seen in anterior and lateral leads • Most often seen in males ages 20-40 • African-American males
Benign Early Repolarization • Look for notch at J-point • ST segment and J-point create a “fish hook” appearance
Pericarditis • May be viral, bacterial or metabolic • Clinical presentation may include chest pain • Often produces ST elevation on ECG
Pericarditis • Clinical presentation • Sharp chest pain • Can be localized • Radiates to base of neck, between shoulder blades
Pericarditis • Pain affected by movement and respiration • Pain improves when patient leans forward • Pain worsens when patient supine
Pericarditis • May produce ST elevation in any lead • May be in all leads • May not be anatomically grouped • J-point notching often present • Fish hook
Medications • Some medications affect the ECG • Digitalis • ST depression • Characteristic sag
Summary • Imitators can produce ST elevation or depression • Imitators can eliminate ST elevation or depression
Summary • Imitators can produce T wave inversion • Imitators can hide T wave inversion