Download
1 / 47
1.46k likes | 4.87k Views
BUNDLE BRANCH BLOCK. Prepared by: DR. Ahmed Omer Bashehri. OBJECTIVES. Anatomy & Physiology of Conductive system. Blood Supply of Conductive System. Patho -physiology of Conduction Disturbances & Their Clinical Significance: BBBs Fascicular Blocks

E N D
BUNDLE BRANCH BLOCK Prepared by: DR. Ahmed Omer Bashehri
OBJECTIVES • Anatomy & Physiology of Conductive system. • Blood Supply of Conductive System. • Patho-physiology of Conduction Disturbances & Their Clinical Significance: • BBBs • Fascicular Blocks • Bi & Tri Fascicular Blocks • Pacemaker Patterns • SVT with Aberrancy • Diagnosis of AMI on top of LBBB
Anatomy & Physiology of Conductive system Normally, cardiac stimulation starts in the SA node from which the stimulus spreads first through the RA & then into LA & so the SA node functions as the normal pacemaker of the heart. The electrical stimulus then spreads to specialized conduction tissues in the AV junction which includes the AV node & bundle of His, & then into the Lt. & Rt. bundle branches which transmit the stimulus to the ventricular muscle cells. The upper part of the AV junction is the AV node & the lower part is called the bundle of His which divides into 2 main branches: the RBB & LBB which in turn subdivided into LAF & LPF.
Anatomy & Physiology of Conductive system ( cont`d ) The electrical stimulus spreads simultaneously down the Lt. & Rt. BBs into the ventricular myocardium by way specialized conducting cells called Purkinje fibers.
Anatomy & Physiology of Conductive system ( cont`d ) • Normal conduction speed through the bundles is about 0.1 seconds & this is the reason the normal width of QRS complex is equal or less than 2.5 small squares.
Anatomy & Physiology of Conductive system ( cont`d ) The 1st part of the ventricles to be stimulated is the Lt. side of ventricular septum & on the normal ECG, this septal depolarization produces a small septal r wave in lead V1 & a small septal q wave in lead V6. Soon after, the depolarization spreads to the main mass of the Lt. & Rt. ventricles by way of LBB & RBB. Since the LV is normally electrically predominant, producing deep S waves in the Rt. chest leads & tall R waves in the Lt. chest leads.
Blood Supply of Conductive System In most individuals the RCA is the most frequent blood supply to the SAN 60 % & AVN 90 % while the LCX supplies the remaining percentage, SAN 40 % AVN 10 % The Bundle of His is supplied from the AV branch of RCA with small contribution from septal perforators of LAD After division of His bundle, the septal perforators of LAD supply the Rt. bundle with collaterals from the RCA & LCX The LAF is supplied from LAD while the proximal portion of LPF receives dual blood supply from nodal artery, generally a branch of RCA, & from LAD. The distal portion of the LPF is supplied from 2 sources: the anterior & posterior septal perforating arteries.
Blood Supply of Conductive System ( cont`d ) N.B: LAF IS VERY SENSITIVE TO ISCHEMIA
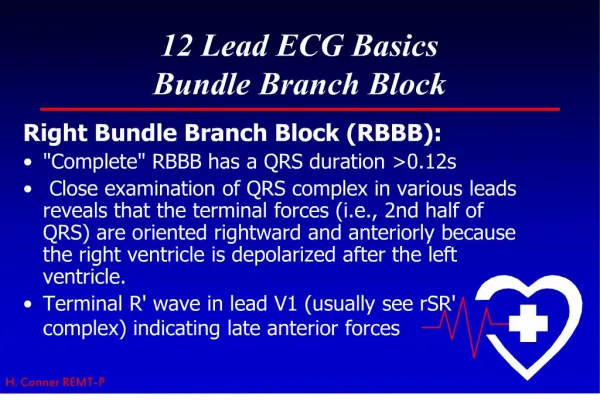
Patho-physiology of Conduction Disturbances & Their Clinical Significance Clearly, RBBB should not affect the septal & LV depolarization so the change in the QRS complex produced is a result of delayed right ventricular depolarization ( 3rd phase ) With RBBB, lead V1 typically shows an r SR` complex with a broad R` wave & lead V6 shows a qRS complex with a broad S wave.
Right Bundle Branch Block First Phase will be normal Second Phase - Normal Third Phase - ? After the left ventricle has completely depolarized, the right ventricle continues to depolarize
Right Bundle Branch Block 1. 2. 3. 1. r wave in V1 q wave in V6 2. S wave in V1 R wave in V6 3. R’ wave in V1 S wave in V6
Patho-physiology of Conduction Disturbances & Their Clinical Significance RBBB also produces 2ry changes ( TWIs in the Rt. chest leads ) which are characteristic finding with RBBB because they reflect just the delay in ventricular stimulation. Clinical Significance: • Normal variant • PE • ASD with Lt. to Rt. shunt • Chronic pulmonary disease with PHT • Valvular lesions as PS • Related to chronic degenerative changes • CAD
Right Bundle Branch Block Criteria V1 or V2 = rSR’ - “M” or rabbit ear shape V5 or V6 = qRS Large R waves Right chest leads: T wave inversion (“secondary changes” since they reflect a delay in depolarization not an actual change in depolarization) Complete RBBB: QRS > 0.12 sec. Incomplete RBBB: QRS = 0.10 to 0.12 sec. Don`t forget the causes of tall R wave in V1……..DDx?
Patho-physiology of Conduction Disturbances & Their Clinical Significance By itself RBBB not require any specific treatment but in acute anterior MI with new RBBB indicate the increased risk of CHB especially when associated with hemiblocks. Conversely to RBBB, LBBB affects the early septal depolarization so the normal pattern is blocked. Thus the 1st major ECG change produced by LBBB is a loss of the normal septal r wave in lead V1 & the normal septal q wave in lead V6. As a result, lead V1 typically shows a wide entirely negative QRS ( QS ) complex & lead V6 shows a tall wide, entirely positive ( R ) wave. Just as 2ry TWIs occur with RBBB they also occur with LBBB.
Left Bundle Branch Block Loss of septal R in V1 and septal Q in V6. • Wide QRS • Negative in V1 • Positive in V6
Left Bundle Branch Block 1. r wave in V1 R wave in V6 2. S wave in V1 R wave in V6
Left Bundle Branch Block Criteria Wide QRS complex V1=QS(orrS )andmayhavea“W”shapetoit. V6 = R or notched R showing a “M” shape or rabbit ears Secondary T wave inversion Secondary if in lead with tall R waves Primary if in right precordial leads
Patho-physiology of Conduction Disturbances & Their Clinical Significance Unlike RBBB, LBBB is usually a sign of organic heart disease & so it may be the first clue to 4 previously undiagnosed but clinically important abnormalities: • Advanced CAD • VHD • HHD • Cardiomyopathy • Related to degenerative changes N.B.: Most patients with LBBB have underlying LVH
RBBB versus LBBB ? ?
Fascicular Blocks Recognition of fascicular blocks on the ECG is intimately related to the subject of axis deviation & surprisingly does not markedly widen the QRS complex. Specifically, LAFB results in marked LAD; LPFB produces marked RAD. LAFB S wave in lead aVF equals or exceed R wave in lead I. Lead a VL usually shows qR complex with rS complexes in inferior leads. LPFB Usually rS complex in lead I & a qR complex in inferior leads. Its diagnosis is by exclusion.
Left Anterior Fascicular Block (LAFB) rS rS qR I III II Initial QRS forces directed rightward (negative in Lead I) and inferiorly (positive in Leads II and III Subsequent predominant forces directed leftward (positive in I) and superiorly (negative in II and III)
Left Posterior Fascicular Block (LPFB) rS qR qR II III I Initial QRS forces directed leftward (positive in Lead I) and superiorly (negative in Leads II and III Subsequent predominant forces directed rightward (negative in I) and inferiorly (positive in II and III)
Bi & Tri Fascicular Blocks Bifasicular block indicates blockage of any two of the three fascicles e.g. RBBB with LAFB produces RBBB pattern with marked LAD; RBBB with LPFB produces RBBB pattern with RAD. Bifascicular blocks are potentiall significant……why? Therefore the acute development of new bifascicular block during acute anterior MI is an important warning signal of possible impending CHB.
SVT with Aberrancy In some cases, a supraventricular tachycardia can present as a wide complex tachcyardia. The brugada criteria were established to distinguish SVT with aberrancy from VT. Steps 1-3 can be helpful in distinguishing VT from an SVT with aberrancy. Step 4 is included as a reference, as in some cases determining a right bundle from left bundle pattern may be helpful in localizing location of the VT (RVOT vs. LV origin).
Brugada Criteria 1) Lack of RS complex in the precordial leads2) When RS complex is present, whether the longest interval in any precordial lead from the beginning of the R wave to the deepest part of the S wave is greater than 100 ms3) Presence of AV dissociation4) Both leads V1 and V6 fulfill criteria for classic VTa) Look for RBBB morphology in V1: - Monophasic R wave in V1 - Notched R wave - QR complex in V1
Brugada Criteria (Cont`d ) b) RBBB morphology in V6 - R to S ratio < 1 (R wave smaller than the S wave) - QSpattern c) LBBB pattern in V1 or V2 - Broad R wave (>0.04s) - Notched downslope in S wave - Onset of R wave to the nadir of the S wave > 0.06 sd) LBBB pattern in V6 - Presence of any Q wave, QR, or QS favors VT Aberrancy with an SVT has two major mechanisms: BBB & WPW preexcitation
Electrocardiographic Differentiation of VT vs. SVT with Aberrancy • Clinical history – if the patient has had an MI in the past?…it is VT until proven otherwise • AV dissociation • QRS morphology • QRS axis • Fusion beat • Capture beat
A-V Dissociation, Fusion, and Capture Beats in VT V1 E F C ECTOPY FUSION CAPTURE Fisch C. Electrocardiography of Arrhythmias. 1990;134.
AMI on top of LBBB (Sgarbossa Criteria ) LBBB is always pathological and can be a sign of myocardial infarction. The criteria (Sgarbossa) that can be used in case of a LBBB and suspicion of infarction are: • ST elevation > 1mm in leads with a positive QRS complex (concordance in ST deviation) (score 5) • ST depression > 1 mm in V1-V3 (concordance in ST deviation) (score 3) • ST elevation > 5 mm in leads with a negative QRS complex (inappropriate discordance in ST deviation) (score 2)
Sgarbossa Criteria This criterion is sensitive, but not specific for ischemia in LBBB. It is however associated with a worse prognosis, when present in LBBB during ischemia At a score-sum of 3, these criteria have a specificity of 90% for detecting a myocardial infarction During right ventricular pacing the ECG also shows left bundle brach block and the above rules also apply for the diagnosis of myocardial infarction during pacing, however they are less specific
أجمل التهاني وأسمى التبريكات المكللة بأجمل باقات الورد المعبقة بنسمات الفل والياسمين والمعطرة بشذى النرجس والرياحين تحملها طيور الحب والنورس نقدمها إلى زميلينا الدكتور / فيصل الصبري والدكتورة / رؤى ياسين بمناسبة الخطوبة وعقبال ما نفرح بزواجكم إنشاء الله