Download
1 / 47
530 likes | 938 Views
Andriy Lepyavko, MD, PhD Department of Internal Medicine № 2. Chronic Obstructive Pulmonary Disease (COPD). Plan of the lecture. Etiology, pathogenesis of COPD Diagnostic criteria Principles of treatment Step-by-step treatment.

E N D
Andriy Lepyavko, MD, PhD Department of Internal Medicine № 2 Chronic Obstructive Pulmonary Disease (COPD)
Plan of the lecture • Etiology, pathogenesis of COPD • Diagnostic criteria • Principles of treatment • Step-by-step treatment
COPD and Bronchial Asthma are the most common diseases of lungs • 4-10 % of adult people are ill with COPD • In Europe 7,4 % of people have COPD • Mortality of such patients is 10 %
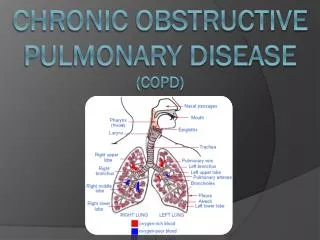
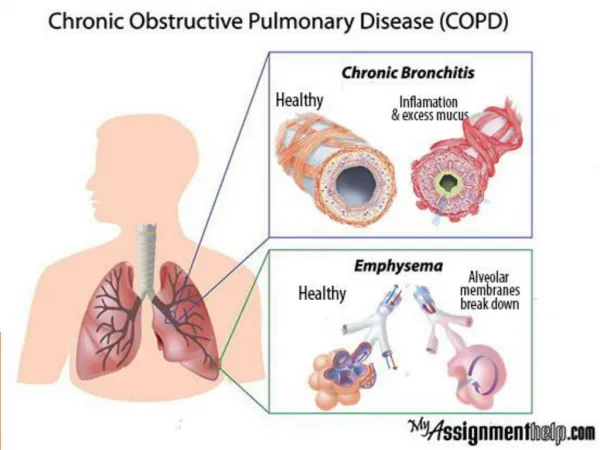
According GOLD 2006 COPD – this is disease which is characterized by combination of clinical signs of chronic obstructive bronchitis (inflammation and narrowing of bronchi) and emphysema (changes of lung tissue structure).
Pathogenesis of COPD • Permanent hyperactivity of parasympathetic nervous system with hyperproduction of acetylcholine, bronchial spasm and hypersecretion of mucus • Insufficiency of adrenal receptors in bronchial walls as the result of deep morphological changes with bronchial hypersecretion, bronchial spasm and cough • Bronchial hyperreactivitywhich is characterized by immune inflammation of bronchioles walls All that lead to: • 1) narrowing of bronchioles; • 2) development of emphysema
Pathophysiology ofCOPD • 1.Hypersecretion of mucus • 2.Dysfunction of ciliary epithelium • 3.Decreasing of air flow in bronchi • 4.Hyperpneumatization of lungs • 5.Disturbances of gases-exchange • 6.Pulmonary hypertension • 7.cor pulmonale
Anamnesis • Severe smoking • Occupational diseases • Family anamnesis
Complaints • Chronic cough is the earliest sign of COPD and arise earlier then dyspnea • Sputum – as a rool in small amount, after cough • Dyspnea – persistent, progressive, becomes worse during physical activity and in severe cases – even if patient is calm
Physical signs • Central cyanosis, emphysematous chest, additional breathing muscles are necessary for breathing • Increasing of breathing rate, decreasing of its deepness, prolongation of expiration • Percussion: decreasing of heart dullness • Auscultation: wheezing, dry rales, heart tones are dull
Methods of investigation of patients with COPD according “GOLD” • Investigation of external breathing (spyrometry); • Bronchodilatation test; • Cytology of sputum; • Blood analysis; • X-ray; • ECG; • Blood gases;
Investigation of external breathing • FVC – max air volume which is expired during forced expiration after max inspiration; • FEV1 (<80 %) • FEV1/FVC (<70 %) • Peak flow (of expiration)
X-ray signs of COPD • Lungs are enlarged • Dyaphragm is located lower than normally • Narrow heart shadow • Sometimes – emphysematous bullas
Bronchodilatation test • Is necessary to find bronchial reversibility • Spyrometry has to be provided before and 15 min after inhalation of 400 mkg of Salbutamol (or 30-45 min – 80 mkg of Ipratropium) • Increasing of FEV1 more than 15 % tells us about reversibility
Principles of treatment of COPD • Increasing of intensivity of treatment in correlation with COPD severity; • Permanent basis therapy; • Individual sensitivity of patients to different medicines leads to necessarity of permanent control; • Inhaled medicines are useful.
Inhaled cholynolytics • Short action – (Ipratropium bromid, Berodual Н) has more slowly beginning but longer action than β2-agonists • Prolonged action – (Thyotropium bromid,Spiriva ) is active for 24 hours
Inhaled broncholytics • agonists of short action(Salbutamol, Fenoterol) – fast beginning of action, but duration – 4-6 hours • 2-agonists of prolonged action (Salmeterol, Formoterol ) are active for 12 hours.
Methylxantines • Theophyllines of prolonged action are useful – Teopec, Teotard.
Glucocorticosteroids • Are useful for permanent basis therapy for patients with COPD III-IV st. • Inhaled GCS areused. • Prednisone may be used only during exacerbation and is not recommended for basis therapy
Inhaled GCS (Beclomethasone, Budesonid, Fluticasone). • Seretid (GCS+Salmeterol) is used in patients with III-IV st. of COPD and oftern exacerbations in anamnesis.