Download
1 / 16
160 likes | 408 Views
Abnormality & Disorders. Abnormality: infrequent in population, violates norms, disability, distress. Abnormality & Disorders. Psychological Disorder: pattern of behavior that: Causes significant distress Causes harm to self or others Interferes with ability to function.

E N D
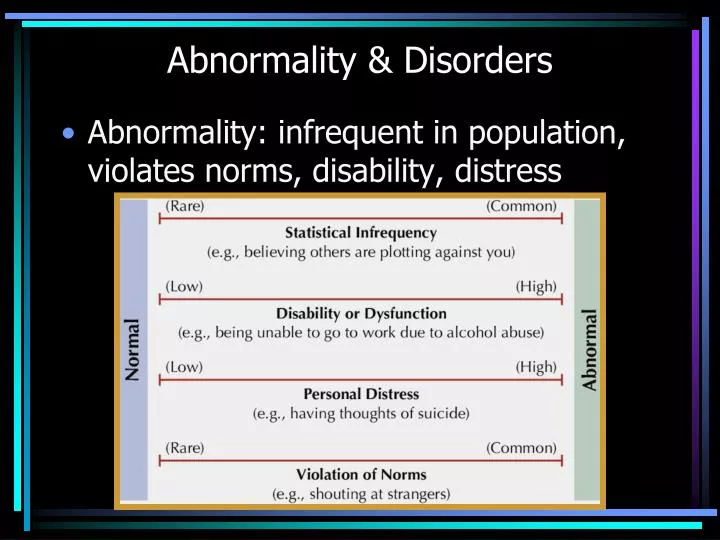
Abnormality & Disorders • Abnormality: infrequent in population, violates norms, disability, distress
Abnormality & Disorders • Psychological Disorder: pattern of behavior that: • Causes significant distress • Causes harm to self or others • Interferes with ability to function
Models of Abnormality • Stress-Vulnerability Model: genetic predisposition to disorder; symptoms brought out during stress • Biological: neurotransmitter function • Evolutionary: exaggerated form of adaptive behavior • Cognitive: faulty thinking
Models of Abnormality • Learning/Behavioral: inappropriate conditioning or modeling • Humanistic: blocked personal growth; poor self-concept • Psychoanalytic/Psychodynamic: unconscious conflict (id, ego, superego) • Sociocultural: cultural beliefs or values
Control vs. Influence • Emotion • Memory • Thinking • Conditioning • Neurotransmitters • Nervous system • Behavior??
Living with a disorder • 22% of people at any given time • Most can be treated successfully • Long-term prognosis: may see alternate periods of normal functioning with periods of disorder – or – management with proper treatment • Recovery?
Stress Psychosomatic disorders: interruption to proper functioning because of overloaded nervous system Prolonged stress creates physical problems Stomach pain, asthma, eczema, hives, migraine headaches, rheumatoid arthritis, high blood pressure, colitis, heart disease, sore muscles (neck, back), indigestion, constipation, chronic diarrhea, fatigue, insomnia, sexual dysfunction Prolonged stress triggers and/or worsens psychological symptoms Related to increased symptoms for mood, anxiety, somatoform, eating, and schizophrenia disorders Extreme stress or trauma can trigger initial symptoms, especially PTSD, dissociative disorders, bipolar disorder, and schizophrenia
Somatoform Disorders Belief of physical illness without actual physical ailment Hypochondiasis: constant worry about illness Somatization Disorder: show of worry about specific symptoms for medical attention Conversion Disorder: unexplained CNS disruption, e.g., paralysis Biological Factors: None Environmental Factors: anxiety, reinforcement during illness, cognitive magnification of bodily changes
Schizophrenia Thought disorder: Interruption to normal thinking / reasoning processes, usually with unexplainable auditory or visual experiences The brain tries to fill in the gaps to make sense but the result does not reflect reality Positive Symptoms (+): incoherence, loose associations, paranoia, clang associations, hallucinations (esp. auditory), delusions of: grandeur, persecution, reference Negative Symptoms (-): loss of normal thought or behavior, catatonia, social withdrawal, inappropriate emotions/affect
Schizophrenia Biological Factors (DP 14:03-15, 18:18-19:50) genetic predisposition (gene combination), disordered brain structures, NT imbalance (too much DA thinking areas, too little DA & glutamate emotion areas) Environmental Factors low support, stress, double-bind parenting, nutrition, drug use (during critical stages of development) Treatment Anti-psychotics for positive symptoms, stress management, social support, family therapy, social training (video)
Prognosis Schizophrenia Maintenance drugs or symptoms for life Psychotherapy to reduce episodes, severity, manage relationships, life skills
Dissociative Disorders Dissociative Amnesia can't recall information related to a traumatic or highly stressful event (selective to incident) Dissociative Fugue State sudden, unexpected travel from home, can't recall their past or personal identity
Dissociative Disorders Dissociative Identity Disorder 2 or more distinct personality states where different states recurrently take control of the host The host’s memory of events experienced as other personalities is dependent on relationship with alters
Dissociative Disorders Biological Factors Not sure; can easily dissociate Environmental Factors High anxiety or traumatic experience Prognosis Amnesia and Fugue often spontaneously recover Dissociative Identity Disorder rarely recover (integration usually unsuccessful) but can manage symptoms, relationships
Other Disorders Impulse control: lacking inhibition of urges Seasonal: related to sunlight, environ. Comorbidity: presence of more than one disorder