Download
1 / 46
630 likes | 2.03k Views
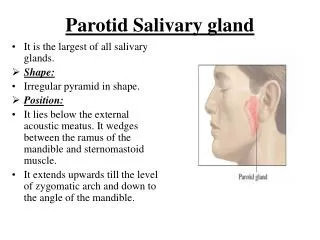
Tumors and Tumor-like Lesions of Salivary Gland. Parotid: Largest major salivary gland Stensen's duct Serous Facial nerve. Submandibular gland Wharton's duct Mucous-Serous Sublingual gland Bartholin's duct, Rivinus ducts Mucous-Serous Small salivary glands Mucous.

E N D
Tumors and Tumor-like Lesions of Salivary Gland
Parotid: Largest major salivary gland Stensen's duct Serous Facial nerve Submandibular gland Wharton's duct Mucous-Serous Sublingual gland Bartholin's duct, Rivinus ducts Mucous-Serous Small salivary glands Mucous MAJOR FEATURES OF SALIVARY GLANDS
Intercalated duct Acinus, serous Striated duct Acinus, mucous
Serous, mucinous glands EM-serous cell
Pleomorphic adenoma (mixed tumor) Papillary cystadenoma lymphomatosa Oxyphil adenoma Sebaceous cell adenoma Benign lymphoepithelial lesion Unclassified Malignant mixed tumor Mucoepidermoid tumor Squamous cell carcinoma Adenocarcinoma Adenoid cystic Trabecular or solid Anaplastic Mucous cell Pseudoadamantine Acinic cell Unlassified Salivary Gland Tumor: Benign vs. Malignant
Salivary Gland Tumors • 2% of head and neck neoplasm • Parotid: 80% overall; 80% benign • Submandibular: 15% overall; 50% benign • Sublingual/minor: 5% overall; 40% benign
Pleomorphic Adenoma (Benign Mixed Tumor) • PA account for 25-30% of all salivary gland tumors. 60-70% of all parotid tumor; 40-60% submandibular gland; 40-70% minor salivary gland tumor. F:M=1.9:1 • PAs are epithelial-derived tumors composed of cells with epithelial and mesechymal-like features. They often display both ductal and myoepithelial differentiation, but less frequently are predominantly ductal or myoepithelial and may mimic monomorphic adenomas, such as myoepithelioma, basal cell adenoma or canalicular adenoma. • Recurrence after surgery: <5%; due to finger-like tumor projections
Irregular, round to ovoid mass Well defined borders In major salivary gland: Incomplete fibrous capsule or unecapsulated. In minor salivary gland: Unencapsulated Homogeneous tan to white cut surface Hemorrhage and infarction on occasion Pleomorphic Tumor: Gross
Pleomorphic adenoma • EPITHELIUM • Anastomosing trabeculae • Ducts • Cysts lined by squamous epithelium • STROMA • Fibrous interlacing bundles • Myxoid areas • Chondroid areas • Myxochondroid areas • Osseous areas • Fibrillar eosinophilic areas
Pleomorphic adenoma: low cellularity, high cellularity, myoepithelial cells, and basal cells predominante
Pleomorphic adenoma: squamous metaplasia and chondrometaplasia
Carcinoma ex Pleomorphic Adenoma • Clinical & radiological features: rapid growth in preexisting lesion of long duration; pain and nerve paralysis; cystic change (CT); microcalcification (CT); regional lymph node enlargement • Pathologic features: elevated mitotic rate; tissue infiltrationm especially perineural invasion; necrosis; microcalcification; lymph node or distant metastasis; sclerosis with entrapment of epithelial elements
Carcinoma ex pleomorphic adenoma Risk of malignancy in pleomorphic adenoma: 5-7%
Warthin’s Tumor (Papillary Cystadenoma Lymphomatosum) -1 • Occurs only in the parotid gland • 2nd most common benign parotid tumor • May be unilateral or bilateral • May occur as multiple lesions either synchronously or metachronously • More common in males (26:1) • More common in smokers • Occurs as a painless, sometimes fluctuant mass
Warthin’s Tumor (Papillary Cystadenoma Lymphomatosum) -2 • May be associated with acute onset of pain and a sudden increase in size (papillary cystadenoma lymphomatosum syndrome) • Retrograde infection • Ear symptoms (tinnitus, deafness, earache) • Facial nerve paralysis • The ability to concentrate sodium pertechnetate (99mTc) is suggestive of Warthin tumor
Rare; 2.3% of salivary tumor 6th decade; M:F=1:1 Parotid: 78% Submandibular: 8% Minor salivary gland: palate, tongue, buccal mucosa Oncocytoma
Mucoepidermoid Carcinoma • MEC:2.8-15.5% of all salivary gland tumors, 12-29% of malignant salivary gland tumors; most common type of malignant minor salivary gland tumors • 53-56% in major salivary gland with 85-88% in parotid • Most frequently seen in 35-65 yrs-old; most common malignant salivary glands in children and adolescens under 20 yrs-old; F:M=3:2 • 44% patients with history of radiation
Mucoepidermoid Carcinoma –Grading (modified from Ellis GL et al) • Parameter (point of value): cystic component of <20% (+2); neural invasion (+2); necrosis (+3); 4 or more mitoses/10 hpf (+3); anaplasia such as nuclear pleomorphism and hyperchroamtism, increase N/C, prominent nucleoli (+4) • Grade: Low (0-4); Intermediate (5-6) and high (7-14) • Note: The grading tends to downgrade MEC. Additional paameters such as aggreesive pattern of infiltration, vascular/lymphatic invsion be included.
Mucoepidermoid Carcinoma, low-grade • The neoplastic cells were arranged into solid nests and islands, there was cyst formation. Mucicarmine stain did demonstrate focal intracellular mucin. The solid growth pattern, focal mucocytes and focal epidermoid cells supports the diagnosis of mucoepidermoid carcinoma. Lack of necrosis, anaplasia, neural invasion and a low mitotic count caused us to give this lesion a low grade designation. Histologic grade is associated with prognosis and these tumors have a favorable prognosis based on both histologic grade and anatomic location. Conservative excision that ensures tumor free margins is adequate therapy.
Adenoid Cystic Carcinoma • A malignant epithelial neoplasm of ductal (lumial) and myoepithelial (abluminal) cells grwoing in cribriform, tubular, solid and cystic patterns More common in parotid gland;most common malignant tumor of intraoral salivary glands ; Female to male ratio, 3:2 • Slow growing tumor; small tumors movable by palpation, larger tumors adherent to skin and soft tissues ;Tenderness and pain ;Facial nerve paralysis ;Mucosal ulceration
Acinic Cell Carcinoma • Acinic Cell Carcinoma is a rare salivary gland cancer, approx. 4% of all minor, and 2-4% of all major salivary gland tumors and approx. 13% of all malignancies of the parotid gland, and are rarely seen in other salivary tissues. • Acinic Cell Tumors are typically slow-growing, low-grade (highly differentiated) neoplasms that appear in all age groups, but are most common in women. Local and multiple recurrences may occur in up to half of patients. The most common sites of metastases are lungs and bone.Many authors consider Acinic Cell Carcinoma patients to have the most favorable outlook of all salivary gland patients, with survivals of 80-85% at 10 years.
Various histologc appearance Recurrent actinic cell carcinoma
Papillary Cystadenocarcinoma of Salivary Gland • The majority of papillary cystadenocarcinomas have a biologic behavior similar to that of a benign neoplasm: recur infrequently,not to metastasize. The tumor lacked basophilic zymogen granules, typical of serous acinar cells. Both benign and malignant tumors often have broad "pushing" lobules with no significant cytologic atypia and high mitotic rate; therefore, classification of such lesions as benign or malignant is based on subjective evaluation. A papillary cystic salivary tumor not readily identifiable as a benign lesion is often regarded as a low-grade carcinoma, particularly with complex branching, bridging, or cribriform pattern.
Mucocele & Ranula Etiology: Trauma Location(s): Lining mucosa. Clinical Features: Raised, bluish, translucent, fluctuant lesion. Microscopic: Chronic inflammation with macrophages surrounding spilled saliva.
Necrotizing Sialometaplasia-1 • Uncommon disease; male:female=1.5-2:1, usually occurs in patients > 40 years old. It most commonly presents with a painful lesion of the hard palate, usually with ulceration. A self-limited condition and it probably results from ischemic changes involving the minor salivary glands and thus can be found in the nasal cavity, gingiva, lip, hypopharynx, maxillary sinus, and major salivary glands. There is a primary form which usually involves the minor salivary glands of the palate and is of unknown etiology.
Necrotizing Sialometaplasia-2 • Histological: the lobular necrosis of the salivary gland tissue, preservation of the lobular architecture, squamous metaplasia of the residual ducts and acini, and temporal variability of the inflammatory cell infiltrate. • The importance in making this diagnosis rests with the pathologist distinguishing this disorder from a malignancy. Squamous cell carcinoma or mucoepidermoid carcinoma of the palate should never be made until necrotizing sialometaplasia is excluded.
Non-Neoplastic Salivary Gland Disease • Many causes of salivary gland enlargement are unrelated to neoplasms. Sarcoidosis, mumps, malnutrition, iodine therapy and hepatic cirrhosis, are well-recognized causes for salivary gland enlargement. The probable autoimmune conditions -- Mikulicz's disease and Sjogren's syndrome are additional salivary gland disease. Probably the most common is sialadenitis secondary to duct obstruction. Although major salivary gland ducts may be obstructed by strictures, scar formation and tumor involvement, an occluding sialolith is the most frequent cause of obstruction.