Download
1 / 17
290 likes | 754 Views
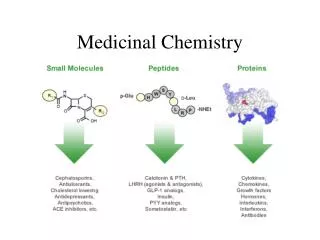
Medicinal Chemistry II 4 th year Pharm Students 1435-2014. Prepared by; Dr. Munjed Ibrahim E-Mail: drabumalik67@gmail.com Tel: 025270000-Ext.; 4268. General Anaesthetics - Introduction. General anaesthesia: loss of sensation with reversible loss of conciousness

E N D
Medicinal Chemistry II4th year Pharm Students1435-2014 Prepared by; Dr. Munjed Ibrahim E-Mail: drabumalik67@gmail.com Tel: 025270000-Ext.; 4268
General Anaesthetics - Introduction General anaesthesia: loss of sensation with reversible loss of conciousness & Depression of defense and muscle reflexes. Anesthetics are depressant drugs that produce a partial or total loss of the sensation. Stages of anaesthesia produced by general anaesthetics • General anaesthesia involves administration of different drugs: • Premedication • Inducing agent(s) • Maintenance agent(s) Slide 18
General Anaesthetics - Introduction • Premedication • Prevention of bradycardia, bronchial secretion, muscle spasm • Benzodiazepines (Diazepam) • Narcotic analgesics • Anticholinergic drugs (Scopolamine) • Skeletal muscle relaxants (CNS) • Inducing agent • Normally an intravenous anaesthetic • Barbituate (thiopentone, methohexitone) • Non-barbituate (propofol, ketamine) • Maintaining anaesthesia • Normally an inhaled gas • halogenated hydrocarbons and ethers • nitrous oxide (and….) Anti-emetic agents may be required post-anaesthesia Slide 19
Mechanisms of anesthesia 1- Blocking the NMDA and glutamate controlled channels.Glutamate or NMDA(N-methyl-D-aspartate) receptors in the CNS are activated by the excitatory AA neurotransmitter glutamic acid. Agonists:This activation opens the channel, allowing K+ to flow to the extra cellular fluid and Na and Ca++ to flow into the nerve cell. The increased intracellular [Ca++] activates the liberation of the (NO), which causes alertness (consciousness).Antagonists:Ketamine blocks NMDA receptors, causes CNS depression (anesthesia) 2- Activation of the inhibitory GABA receptor controlled channel. Binding of GABA (inhibitory transmitter) to their receptors will open the Cl- channel, leading to the influx of Cl- and hyper- polarization of the neuron. Halothane and isofluraneinhibit the synaptic destruction of GABA, thereby increasing the GABA-ergicneurotransmission. Benzodiazepinesand barbiturates: Inhance GABA opening Cl channels
Depending on route of administration,general anesthetics are classified 1- Inhalation (pulmonary) Anesthetics: - Gases or vapors of volatile liquids that inhaled in a mixture with air or O2. 2- Intravenous Anesthetics: Agents are psychologically well tolerated. They are quite useful as induction agents for inhalation anesthesia. 3- Combination Anesthesia: Combinations of medications is preferred to broaden the therapeutic range. Moreover, minimal doses of several substances are administered for particular goals of anesthesia.
Inhaled anesthetics • Nitrous oxide:N2O, laughing gas • - A colorless gas, exerts low anesthetic effect. • - It is mixed with oxygen and ether or halothane, as deep anesthesia cannot be achieved with it alone. • - Has good analgesia & minimal toxicity, it has poor m. relaxant effect. • Dosage: • For induction, 70% nitrous oxide with 30% oxygen for 2 to 3 minutes. • For maintenance, 30 to 70% nitrous oxide with oxygen. • 2.Non-halogenated Hydrocarbons: • They have a tendency to produce cardiovascular toxicity. • The longer chain of the hydrocarbon, the higher the potency. • Cyclopropane is • colorless, explosive and flammable, may cause laryngospasms. • the only hydrocarbon still in use. • mixed with oxygen (15 – 30% Cyclopropane) for medical purposes. • In contrast to nitrous oxide, its concentration of 20% can produce anesthesia.
SAR of the Volatile General Anesthetics ALKANE / CYCLOALKANE • 1. The potency of alkanes, cycloalkanes, and aromatic hydrocarbonsincreases in direct proportion to the number of carbon atoms in the structure up to a cutoff point. • In the n-alkanes, the cutoff number is 10. While in cycloalkanes, 8 • 2. There is a positive correlation between anesthetic potency and solubility in olive oil. • 3. Thecycloalkanes are more potent anestheticsthan the straight chain analog with the same number of carbons. • For example, the MAC of cyclopropane in rats is about one fifth of the MAC of n-propane.
3. Halogenated hydrocarbons Effect of halogenation / ether halogenation: Addition of a halogenreduce or eliminate flammability, and increase potency. Higher atomic mass halogens increasedpotency compared to lower atomic mass halogens. For the n-alkane series, fully saturating the alkane with fluorineabolished activity except when n equaled one. When n was 2 – 4 Cs the highest potency was seen when the terminal carbon contained one H(CHF2(CF2)nCHF2). When n was greater than 5 carbons the potencydecreased in this series. Rate of metabolic defluorination: methoxyF > enF = sevoF >isoF > desF > halothane
Halothane • Chemical Name; 2-bromo-2-chlorol-1,1,1-trifluoroethane • It is noninflammable liquid with a characteristic sweet odor. • The presence of three fluorine atoms, increases potency, volatility and chemical stability. • The induction of and recovery from anesthesia are rapid. • Halothane reduces peripheral vascular resistance. It is a poor muscle relaxant. • Mostly halothane is eliminated as intact. However, about 20% is metabolized to trifluroacetic acid. • The trifluoroacetyl chloride metabolite is electrophilic and can form covalent bonds with proteins leading to immune responses and halothane hepatitis upon repeated use.
4. Halogenated ethers. Polyfluorinated ethers have analgesic and muscle-relaxing properties but are more difficult to control. In addition, some are inflammable. • Enflurane : • Name: 2-chloro- I,I ,2-trifluoroethyl difluoromethylether • Noninflammable liquid, mixed with various amounts of O2 &N2O • Its advantage over halothane is the more rapid induction & recovery. • Arrhythmias are observed less frequently. • It has a low frequency of nephrotoxicity due to low [F-] released from metabolism. (Only 2% is metabolized to fluoride ions and fluoromethoxydifluoroaceticacid) F2HCOCF2CClFOH →F2HCOCF2COOH + F- Drug interaction: INH which facilitate its deflourination, renal damage occurs • Drug toxicity: • ↑ doses it produces convulsions; not used in patients with epilepsy. • Enflurane relaxes the uterus; not used as anesthetic during labor.
Isoflurane:1 -chloro-2,2,2-trifluoethyl difluoromethyl ether. It is noninflammable liquid with a faint odor. It has a low blood/gas distribution coefficient, which leads to rapid recovery from the anesthesia. Only 0.2% of the drug is metabolized to F- and trifluoroacetic acid, therefore kidney, liver and myocardial functions remain intact. The (+) isomer was found to be 53% > potent than the(-) isomer. It is the best general anesthetic so far. Isoflurane is a structural isomer of enflurane.
Intravenous Anesthetics Intravenous anesthetics are nonexplosive solids. They produce rapid loss of consciousness but insufficient anesthesia. So, they are seldom used alone. Administration of oxygen is recommended, particularly with barbiturates and thiobarbiturates. Propofol (Deprivan) 2,6-Di-isopropylphenol • Propofolis a short acting anesthetic that act via enhancing the GABA-ergic neurotransmission in the CNS. It binds allosterically to GABA receptor at a site different from that of benzodiazepines. It achieves hypnosis in one minute & lasts for 5 minutes. • Maintenance of anesthesia is achieved with volatile anesthetics or additional doses of it. • It is formulated as 1 or 2% emulsion in soybean oil or glycerol. • It is more, effective than thiopental. Rarely associated with vomiting. • Metabolism proceeds rapidly via glucuronide and sulfate conjugation in liver.
Ketamine • 2-(2-Chlorophenyl)-2-methylaminocyclohexanone • Ketamine hydrochloride is a very potent, rapidly acting anesthetic agent. • The S (+) ketamine is two to three times more potent than the R (-) ketamine as an analgesic. • Its duration of action is relatively short (10-25 minutes). • It produces anesthesia by blocking the NMDA controlled channels. • ketamine is suitable for diagnostic purposes and for surgical procedures that do not require muscle relaxation. • Patients older than 16 will often (27%) have wild dreams and hallucinations during emergence, that may last for 24 hours and so it is only indicated for children less than 16 years old.
The termination of action is due to redistribution from the brain into other tissues. • In the liver ketamine is metabolized into norketamine(active metabolite), which account for the longer effect of this anesthetic. It is also conjugated with glucuronic acid. [O]
Ultrashort-acting barbiturates: - Used to produce rapid unconsciousness for surgical and basal anesthesia (induce anesthesia). The induction is very rapid. The long side chain substitution at position-5 is an essential feature for increasing lipid solubility and hence the rate of passing through the BBB. There is an inverse correlation between the total number of carbon atoms substituted on the 5 position and the duration of action a- Thiopental sodium • It is the most widely used ultrashort-acting barbiturate. The presence of sulfur in thiopental increases lipid solubility and facilitates its entry to the brain. • Its short duration of action is due to partitioning from the brain into body fat. It is metabolized by oxidative desulphurization
b- Methohexitalsodium • It is N-methylated barbiturate that has pKa of 8.4, versus 7.6 for the non-methylated compound. • This pKa value increases the concentration of the lipid-soluble free acid form at the physiological pH. • N-methylation decreases duration of action. • The compound also has extensive hydrophobic character because the long unsaturated side chains (9-Cs). • Overall, it can rapidly penetrate the CNS after IV injection and then redistribute rapidly to other body sites and undergo rapid metabolic inactivation. • Finally, it has an accessible site of metabolic inactivation, the CH2 α to the triple bond.
Benzodiazepines -Benzodiazepines alone can not produce surgical anesthesia. However, some benzodiazepines are used to induce anesthesia. e.g: Medazolam maleate Adjuvant to general anesthesia 1.Narcotic analgesics: such as morphine and meperidine to reduce anxiety . 2.Sedatives: such as benzodiazepines, to produce sedation and reduce anxiety. 3.Anticholinergics: such as scopolamine, to inhibit excessive respiratory secretion. 4.Skeletal muscle relaxants: such as succinylcholine and vencuronium to relax the muscles for optimum surgical working conditions.