Download

1 / 14
160 likes | 867 Views
Neurogenic Bladder Neurogenic Bowel LE Weakness. Neurogenic Bladder: Spinal Cord Lesions. Urge incontinence Bladder empties too quickly and too frequently External sphincter may have paradoxical contractions Detrusor-sphincter dyssynergia

E N D
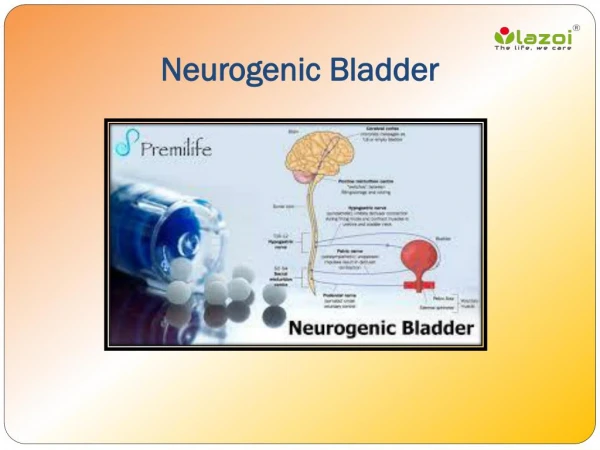
Neurogenic Bladder Neurogenic Bowel LE Weakness
Neurogenic Bladder: Spinal Cord Lesions • Urge incontinence • Bladder empties too quickly and too frequently • External sphincter may have paradoxical contractions • Detrusor-sphincter dyssynergia • Both the bladder and external sphincter become spastic at the same time • Even though the bladder is trying to force out urine, the external sphincter is tightening to prevent urine from leaving.
Neurogenic Bladder • Intermittent catheterization is the factor most responsible for the nearly normal life span of patients with spinal cord injuries. • In this group, urinary tract infection is no longer the leading cause of death.
Intermittent Catheterization Program • Balanced bladder • Volume of residual urine ≤ 1/3 x volume of voided urine • Initiated if the residual volume is greater than 100 mL or if the voided volume exceeds 400 mL • Every 4 hours initially and then every 6 hours for 24 hours
Intermittent Catheterization Program • Ideally, the amount drained each time ≤ 400-500 mL • If catheterization is performed every 6 hours and the amount drained is 700 mL, increase the frequency of catheterization to every 4 hours to maintain the volume drained at 400-500 mL.
Intermittent Catheterization Program • Potential advantages: patient autonomy, freedom from indwelling catheter and bags, unimpeded sexual relations • Potential complications: bladder infection, urethral trauma, urethral inflammation, stricture • Long-term use of intermittent catheterization appears to be preferable to indwelling catheterization
Bladder Training • Relearning how to urinate • Urge incontinence and sensory urge symptoms (though the bladder is not full, it is signaling that it is time to void) • Self-education, scheduled voiding with conscious delay of voiding, and positive reinforcement
Bladder Training • Requires the patient to resist or inhibit the sensation of urgency and postpone voiding. • Patients urinate according to a scheduled timetable rather than the symptoms of urge. • Useful in young women but is difficult to implement in cognitively impaired persons
Others • Crede method • applying external pressure on the bladder to induce emptying • Valsalva maneuver • forcibly exhaling against the closed glottis
Neurogenic Bowel • Spastic / Reflexic / UMN bowel • Impulses are interrupted when a SCI is at the cervical or thoracic level. • SC can still guide bowel reflexes. • Even though you do not feel the need to have a BM, your body's reflexes can do it automatically. • When the bowel becomes full, a BM occurs but in between BMs your anal sphincter stays tight.
Neurogenic Bowel • Flaccid / areflexic / LMN bowel • Happens when the injury is at the lumbar or sacral area • Injury decreases the peristalsis and the reflex control of your anal sphincter. • You cannot feel that you need to have a BM and your anal sphincter may not be able to hold BM in. • The sphincter does not close tightly enough, so BM leaks out.
Neurogenic Bowel • Improvement in mobility and activity levels in affected individuals improves the potential of lessening constipation and fecal impaction. • Improve toileting and transfer techniques goal of improving independence potentially lessening fecal incontinence
Neurogenic Bowel • Regular emptying • Fixed schedule for bowel training • Every other day in most cases
LE Weakness • Clothes modification • Dresses or skirts > pants or shorts • Flip flops to sandals • Home modification • Grab bars in a shower • Transfer bedroom to first floor