Download
1 / 29
300 likes | 325 Views
Learn about local drug delivery in SFA treatment, dosing considerations, and patient outcomes. Review case studies and guidelines for device selection.

E N D
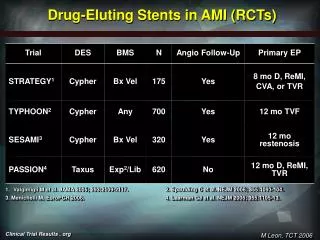
SCAI 2019May 22, 2019Are Drug Eluting Stents the Future of SFA Treatment? SahilA. Parikh, MD, FACC, FSCAI Associate Professor of Medicine Director, Endovascular Services Center for Interventional Vascular Therapy New York-Presbyterian Hospital Columbia University Irving Medical Center Columbia University Vagelos College of Physicians and Surgeons
Disclosures Within the past 12 months, I or my spouse/partner have had a financial interest/arrangement or affiliation with the organization(s) listed below. Affiliation/Financial Relationship Company • TriRemeMedical, Shockwave Medical, NIH, Surmodics, Silk Road Medical (CEC); Boston Scientific (DSMB) • Terumo, Abiomed • Abbott, Boston Scientific, Medtronic, CSI, Philips • Grant/Research Support • Consulting Fees/Honoraria • Advisory Board
Drug “Coated” Balloon Administration Drug Eluting Balloon Drug Eluting Stent Drug Coated Stent Modes of Local Endovascular Drug Delivery Drug release Target site Endovascular modalities tissue FAST CONTROLLED/ SUSTAINED Distribution Clearance FAST ≈EFFECT FAST
Typical DCB Curve Dosing ConsiderationsBalancing Safety and Efficacy TOXIC EFFECT 100 IMPROVE EFFICACY (overlap restenotic cascade) Typical DES Curve THERAPEUTIC WINDOW Arterial Paclitaxel Concentration (ng/mg) REDUCE COMPLICATIONS 5 1 NO EFFECT 0 0 25 50 75 100 Time (Days)
SCAI AUC and FP PVI: 2017 Update Klein AJ et al. Catheter CardiovascInterv. 2017;90(4):E90-E110.
SCAI Consensus Guidelines for Device Selection in FP PVI Device Selection as DEFINITIVE Therapy Feldman DN et al. Catheter CardiovascInterv 2018.
ACC/AHA AUC DES and DCB are both APPROPRIATE for SFA lesions of any length
5-year Primary Patency (PSVR < 2.0)Zilver PTX vs. Standard Care 66.4% Zilver PTX p < 0.01 log-rank Optimal PTA+ BMS 43.4% At 5 years, Zilver PTX demonstrates a 41% reduction in restenosis compared to standard care Source: Dake M. The Zilver PTX randomized trial of paclitaxel-eluting stents for femoropopliteal artery disease: 5-year results. Presented at: VIVA 2014: Vascular Interventional Advances Conference; November 4-7, 2014; Las Vegas, Nevada.
Zephyr Registry: Real World Support for Zilver PTX and Predictors of Restenosis LENGTH >160MM MLA <12mm2 EEM area <27mm2 Lida, et al. JACC: CI Volume 8, Issue 8, July 2015, Pages 1105–1112
Patient Flow 852 screened 328 ineligible 61 general inclusion/exclusion criteria 267 angiographic criteria 59 in sub-studies (Eluvia only) Randomized Trial 465 randomly assigned (2:1) 309 assigned to Eluvia 156 assigned to Zilver PTX 4 withdrew consent 6 died 9 withdrew consent 6 died 146 in full cohort analysis at 12 months 142 clinical visit follow up at 12 months 294 in full cohort analysis at 12 months 282 clinical visit follow up at 12 months Gray WA, Lancet 2018.
Baseline Patient Characteristics Gray WA, Lancet 2018.
Baseline Lesion Characteristics Gray WA, Lancet 2018. Angiographic Core Laboratory Data
Effectiveness I Primary Patency at 12 Months Eluvia (N=309) Zilver PTX (N=156) Δ (95% CI) Treatment Difference for Primary Patency p value 86.8%(243/280) 77.5%(110/142) 9.3% (1.4%, 17.3%) 0.0144 Superior primary patency for Eluvia vs Zilver PTX IMPERIAL Trial: A global randomized controlled multi-center trial with 2:1 randomization of the Eluvia™ Drug-Eluting Stent against Cook Medical’s Zilver™ PTX™ Stent, single-blind, non-inferiority design; independent core lab adjudication. Superiority determined in a post hoc analysis that was specified prior to unblinding. 12-Month Primary Patency rate of 86.8% in the Eluvia arm vs. 77.5% in the Zilver PTX arm (p-value = 0.0144). Primary patency defined as duplex ultrasound PSVR ≤2.4, in the absence of clinically-driven target lesion revascularization or bypass of the target lesion, as assessed by the DUS core lab. Gray WA, Lancet 2018.
Effectiveness I Primary Patency at 12 Months Kaplan-Meier Analysis of Primary Patency 0 1 2 3 4 5 6 7 8 9 10 11 12 13 Error bars are 95%CI. Primary patency defined as duplex ultrasound PSVR ≤2.4, in the absence of clinically-driven target lesion revascularization or bypass of the target lesion, as assessed by the DUS core lab. Gray WA, Lancet 2018.
Safety • Non-inferior MAE rate for Eluvia vs Zilver PTX • Eluvia CD-TLR and stent thrombosis rates ~50% less than Zilver PTX • 6 cases of positive remodeling in Eluvia arm (2.1%) • All 6 lesions patent at 1 year • None had TLR or stent thrombosis Clinical Events Committee-adjudicated adverse events included MAE and stent thrombosis. Potential stent fractures were identified by radiography and verified by the angiographic core lab. Stent-based fracture rate calculation based on 319 implanted Eluvia and 197 Zilver PTX stents. MAE, major adverse events; CD-TLR, clinically-driven target lesion revascularization. Gray WA, Lancet 2018.
IMPERIAL Summary of Deaths: RCT (2:1 randomization) CEC, Clinical Events Committee. *The CEC considered all deaths cardiac unless an unequivocal non-cardiac cause could be established. Gray, WA LINC 2019
IMPERIAL Diabetic Cohort I Primary Patency at 12 Months 180 patients had medically-treated diabetes (116 Eluvia & 64 Zilver PTX) Kaplan-Meier Estimate Primary Patency Rate (%) 87.4% 100% 80% 80.2% 60% 40% 20% 0% Months Since Procedure 0 1 2 3 4 5 6 7 8 9 10 11 12 13 Log-rank p= 0.2905 Observed Rate: 84.6% (88/104) Eluvia vs 79.3% (46/58) Zilver PTX Primary patency defined as duplex ultrasound PSVR ≤2.4, in the absence of clinically-driven target lesion revascularization or bypass of the target lesion, as assessed by the DUS core lab. Müller-Hülsbeck S, LINC 2019
IMPERIAL Eluvia Baseline CTO IPrimary Patency at 12 Months Primary Patency Rate (%) 83.9% CTO 100% 90.6% Non-CTO 80% 60% 40% 20% 0% Months Since Procedure 0 1 2 3 4 5 6 7 8 9 10 11 12 13 Log-rank p= 0.0762 Kaplan-Meier estimate. Primary patency defined as duplex ultrasound PSVR ≤2.4, in the absence of clinically-driven target lesion revascularization or bypass of the target lesion, as assessed by the DUS core lab. Vermassen, F. CX 2019.
IMPERIAL Eluvia Calcified Lesions IPrimary Patency at 12 Months Primary Patency Rate (%) 89.2% Moderate/Severe 100% 87.0% None/Mild 80% 60% 40% 20% 0% Months Since Procedure 0 1 2 3 4 5 6 7 8 9 10 11 12 13 Log-rank p= 0.569 Kaplan-Meier estimate. Primary patency defined as duplex ultrasound PSVR ≤2.4, in the absence of clinically-driven target lesion revascularization or bypass of the target lesion, as assessed by the DUS core lab. Vermassen, F. CX 2019.
Primary patency defined as duplex ultrasound PSVR ≤2.4, in the absence of clinically-driven target lesion revascularization or bypass of the target lesion, as assessed by the DUS core lab. Long Lesion Effectiveness I Primary Patency at 12 Months • Kaplan-Meier estimate: 87.9% at 12 months • Observed rate: 87.0% (40/46) Primary Patency Rate (%) 100% 80% 87.9% 60% 40% 20% 0% Months Since Procedure 0 1 2 3 4 5 6 7 8 9 10 11 12 13 Gray WA, VIVA 2018
IMPERIALPharmacokinetics Sub-study (N=13) • All patients treated with Eluvia • Plasma paclitaxel unquantifiable (<1 ng/mL) in all 13 patients at >10 minutes post-implantation • 1-year mortality 0% Plasma paclitaxel measured at 10 min, 30 min, and 1, 2, 3, 4, 6, 12, 24, 48 hours post-implant. Gray WA, Lancet 2018
SFA Patency Decreases with Lesion Length for PTA and “Conventional Stenting” but less so for Newer Technologies Including Vascular Mimetic Implants and Drug Delivery Conventional PTA Nitinol Stents VMI/Covered Stents/DCB/DES Adapted from: Gray B. CCI. 2011
Do the patency data give us a clue for an algorithm? • PTA/stents • Femoral-popliteal 55-75% • Surgical reconstruction • Femoral-popliteal 65-80% • Femoral-tibial 60-75%
Since the VIVA VLF…. • Signal of Mortality Identified in 3 Data Sets • Data should be interpreted with caution especially because “the specific cause and mechanism of the increased mortality is unknown.” • “[B]ecause of this concerning safety signal, we believe alternative treatment options should generally be used for most patients.” • Convening FDA Panel in June, 2019
March 1, 2019 Drug-Eluting Stent Implantation and Long-Term Survival Following Peripheral Artery Revascularization Eric A. Secemsky, Harun Kundi, Ido Weinberg, Marc Schermerhorn, Joshua A. Beckman, Sahil A. Parikh, Michael R. Jaff, Jihad Mustapha, Kenneth Rosenfield and Robert W. Yeh http://www.onlinejacc.org/content/early/recent
Long-Term Survival after Peripheral DES • *No difference in survival in adjusted analyses • CLI: Adjusted HR 0.97; 95%CI, 0.92-1.03; P = .32 • Non-CLI: Adjusted HR 1.01; 95%CI, 0.91-1.13; P = .80 CLI Non-CLI
PCR Statement on Interventions withDCB • What is Known: Current Evidence withDCB? • As for any meta analysis, the Katsanos analysis has major inherent methodological limitations that prevent reliable interpretation of primary findings, theseinclude: • Study level rather than patient leveldata • Limited long-term data: >80% loss of patients at 4-5 years (3/28 trials), 45% are DES and High drop out rates within trials (>35% loss toFU) • Unmeasured crossovers and re-interventions, and unknown additional PTXexposure • Lack of adjudication of cause ofdeath • Errors in published death rates with subsequentcorrections • Lack of a plausible or reproducible doseresponse • At least 4 new patient-level analyses and a large-scale claims data analysis have failed to replicate the results of the meta analysis withDCB • Coronary DCB applications are not associated with a long-term safetysignal • There is currently no strong evidence of a mortalitysignal Courtesy: Alexandra Lansky, MD
PCR Statement on Interventions withDCB • PCR Position onDCB • Although the results of the meta analysis are not conclusive, they cannot be ignored due to the mortality implications and the lack of high quality long-term safetydata • PCR acknowledges the need for a more reliable industry-wide patient level(DCB • only) pooled analysis, expected to be presented at the upcoming FDA panel on June 19/20 • PCR strongly encourages resuming the previously suspended prospective randomized DCB trials (SWEDPAD and BASIL 3) under careful adjudication and safety oversight as these will provide the evidence necessary to address the safety ofDCB • Until more robust data to the contrary, there is currently no strong evidence to justify changing clinical practice and clinicians should continue to use bestjudgment Courtesy: Alexandra Lansky, MD