Download
1 / 61
640 likes | 898 Views
Peri-Operative Management of Drug Eluting Stents. Stephen T. Thew, MD, FACC Heart Clinics Northwest. Balance. Bleeding Stent Thrombosis. Outline/Highlights. Timing of elective surgery What to do with medications Stopping anti-platelet meds When to restart

E N D
Peri-Operative Managementof Drug Eluting Stents Stephen T. Thew, MD, FACC Heart Clinics Northwest
Balance Bleeding Stent Thrombosis
Outline/Highlights • Timing of elective surgery • What to do with medications • Stopping anti-platelet meds • When to restart • Post operative concerns
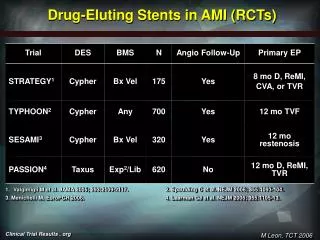
Timing of Surgery Post-Stenting • Bare Metal Stents • Wait 30-45 days for elective surgery • But do it prior to 6 months (or wait > 1 yr) • Drug Eluting Stents • Wait at least 6 months for elective surgery • Ideal - 1 year for elective surgery (??)
Anti-platelet medications • If possible continue all anti-platelet medications • If Plavix (P2Y12) must be stopped do so 5-7 days before surgery and re-start ASAP with 300-600mg bolus • REALLY try to continue aspirin, if stopped do so 5 days before and restart ASAP
Anti-platelet medications • Consider “bridging therapy” with IV administration of IIb/IIIa inhibitor (short half-life) in certain situations • If bridging, start IV IIb/IIIa 2-3 days prior to surgery
Post operative concerns • Close monitoring for bleeding • Chest pain, hypotension, tachycardia all need very prompt attention • Elective surgery should be done at hospital with 24 hour availability of PCI capable cath lab
Peri-op DES: Scope of the Problem • In the US over 600,000 percutaneous coronary interventions (PCI) are done every year • The majority of PCIs involve drug eluting stent placement
Peri-op DES: Scope of the Problem • Dual Anti-Platelet Therapy (DAPT) includes aspirin in addition to a P2Y12 inhibitor (Plavix, Prasugrel, Brilinta, Ticlid) • Following Drug-Eluting Stent (DES) placement, DAPT is recommended for 12 months by ACC/AHA guidelines
Peri-op DES: Scope of the Problem • About 5% of patients undergoing PCI will need non-cardiac surgery within 1 year • About 30,000 procedures annually • Roughly 1% of elective non-cardiac surgery pts. had PCI in the preceding year
Peri-op DESWhat Problems are There? • Increased risk of myocardial infarction • Risk of stent thrombosis • Increased risk of bleeding due to DAPT • Migration of the stent ? • Interference with diagnostic/imaging studies?
Why do Cardiologists have a love affair with DES? • Because they work so well • Work well for what? • Compared to what? • Are there alternatives besides DES?
Brief history of Coronary RevascularizationSurgical Bypass (CABG) • Prior to the 1960s angina was treated with Nitroglycerin • Vineberg procedure had been occasionally used (LIMA grafted directly to the anterior wall myocardium) • 1967 the first CABG was performed at the Cleveland Clinic – an SVG placed to LAD
Brief history of Coronary RevascularizationLimitations of CABG • Surgery required • Prolonged recovery times, in hospital and at home • Repeat procedures can be done, but limited by available conduit, increased morbidity and again prolonged convalescence
Brief history of Coronary RevascularizationBalloon Angioplasty (PTCA) • In 1977 Andreas Gruentzig preformed the first balloon angioplasty in Zurich, Switzerland • Recovery time was minimal, cost was lower, repeat procedures were more practical than re-do CABG
Brief history of Coronary RevascularizationLimitations to PTCA Complications • Acute vessel closure • Dissection • Intra-coronary thrombus • Emergent CABG Durability • Restenosis • Elastic Recoil • Intimal Hyperplasia
Brief history of Coronary RevascularizationCoronary Stenting • In 1994 the FDA approves the use of coronary stents • By the late 1990’s about 85% of coronary interventions utilized stents • Restenosis reduced from 30-40% to 20-30% • Many of the limitations of PTCA were treated/prevented with stents
Brief history of Coronary RevascularizationPTCA limitations now treated by stents Complications • Acute vessel closure • Dissection Durability (Restenosis) • Elastic Recoil – essential resolved • Intimal Hyperplasia – actually worsened • Net effect was still significant reduction in restenosis
Brief history of Coronary RevascularizationLimitations of Stents Stent Thrombosis • Ticlid in addition to aspirin markedly reduced SAT • Formed the concept of DAPT • Plavix (clopidogrel) replaced Ticlid in late 1990’s Durability – (Restenosis) • Elastic recoil resolved, but neointimal hyperplasia got worse • Restenosis rates were 20-30% • Small Vessels, Diabetics, diffuse disease all had even higher restenosis rates
Brief history of Coronary RevascularizationDrug Eluting Stents • 2003 the first DES is approved by FDA • DES deliver locally, a high dose of a chemotheraputic agent to inhibit neo-intimal growth • Restenosis rates dropped to around 4-5%
Why Cardiologists Love DES • PCI reduces mortality and morbidity in acute coronary syndromes • PCI is effective in controlling anginal symptoms • Patient recovery time is short • Essentially unlimited future procedures can be preformed if needed • Long term durability is very good
Limitations of Drug eluting stents • Increased, but later, stent thrombosis in DES • Late (>30 days) • Very Late (>1 year) • Inhibition of neo-intimal growth also inhibits endothelial formation inside the stent • Long term (12 month) Plavix was recommended
In-stent Restenosis/Endothelialization • Bare-metal stents have essentially complete endothelialization at 4 – 6 weeks • DES at 180 days may still have some incomplete endothelialization
Stent Thrombosis • Stent thrombosis • Acute –first 24 hours • Sub-acute – first month • Late – first year • Very late - > 1 year • Overall stent thrombosis rate is 1-2 % in first year • Continues to be a major concern
Stent Thrombosis • During surgery there is a hypercoaguable state induced • Increased inflammation and platelet activation • A greater degree of hypercoaguability is seen from surgery than during an MI
Stent Thrombosis • Post surgery rise in thrombogenic risk - increased catecholamine release - increased platelet aggregation - decreased fibrinolysis
Stent Thrombosis • Discontinuation of aspirin leads to a ‘rebound’ effect
Anti-Platelet Agents in Addition to Aspirin Oral • Ticlid • Plavix • Effient • Brilinta IV • ReoPro • Integrlin • Aggrastat
Oral Anti-Platelet AgentsP2Y12 Inhibitors or ADP Receptor Inhibitors Thienopyridines • Ticlid (ticlopidine) • Plavix (clopidogrel) • Effient (prasugrel) Non-thienopyridines • Brilinta (ticagrelor) • Peak inhibition in just 2 to 4 hours
Anti-Platelet AgentsIV - P2Y12 Inhibitors • Currently – none available • Cangrelor is being studied with PCI • IV administration, 3 to 5 minute half life • Was studied in BRIDGE for pre-op use
IV Anti-Platelet MedicationsGlycoprotein IIb/IIIa Inhibitors ReoPro (abciximab) • Monoclonal anti-body, irreversible binds platelet • Reverse with platelet infusion Aggrastat (tirofiban) Integrlin (eptifibatide) • Synthetic peptides, competitive binding to platelet • Platelet transfusions don’t help – (out competed) • Short ½ life – gone in 2 to 4 hours
Dual Anti-Platelet Therapy (DAPT) Aspirin and a P2Y12 inhibitor Duration: 4 weeks following bare metal stent 12 months following DES 12 months following MI Continuation of aspirin indefinitely
Bleeding Risk During Surgery • Burger, et al – 49,000+ patients, increased bleeding by 1.5, but mostly ‘nuisance’ bleeding • Intracranial procedures did have increased fatal bleeding • TURP may have increased severity level of bleeding
Bleeding Risk with Surgery • There is a decrease in CVAs during CEA with pts on aspirin • Better patency of grafts in CABG and vascular by-pass in patients on aspirin • Increased need for blood products, but no increased mortality in CABG patients on Plavix and aspirin
Bleeding Risk with Surgery • Burger, et al – 49,000+ patients • Stopping aspirin had higher cardiac, cerebral and peripheral vascular events
Surgical Risk and Timing • Non cardiac surgery done less than 6 weeks after PCI has the highest mortality • The single biggest predictor of stent thrombosis is discontinuation of anti-platelet therapy
Surgical Risk and Timing • Retrospective study – Ontario, Canada • ONLY elective surgeries • Increased MACE when <45 days • Bare-metal – optimal time 46 – 180 days • DES – optimal time >180 days • > 1 year and risk has plateaued, is no higher than 2-10 years post PCI Wijeysundera, et al
Surgical Risk and Timing • At > 1 year since PCI the risk approximates that of a intermediate non-revascularized patient with 1 or 2 clinical risk factors Wijeysundera, et al
Peri-op Management of DES • Currently no definitive standard of care, mostly expert opinion • Without good prospective data, management is carried out on individual case basis • Length of stent, location, bifurcation, multi-vessel
Strategies for Peri-op Management of DESELECTIVE SURGERY • Elective surgery should be delayed at least until 6 months post DES • Ideally postponed 1 year post DES • P2Y12 - if stopped - 5 to 7 days pre-op, continue aspirin if at all possible • Resume P2Y12 ASAP with 300 or 600mg loading dose
Strategies for Peri-op Management of DES • “Bridging Therapy” with GP IIb/IIIa inhibitor • Has NOT been rigorously studied • Integrlin or Aggrastat, NOT ReoPro • Stop Plavix 5-7 days pre-op • Admit 2-3 days pre-op and start IIb/IIIa • Continue aspirin throughout if possible • Restart Plavix as soon as possible post-op
Strategies for Peri-op Management of DESURGENT SURGERY • Urgent-Emergent surgeries have 4-fold higher mortality
Strategies for Peri-op Management of DESURGENT SURGERY • Continue DAPT if possible - stent thrombosis risk is high • Closed/confined space – intracranial, spinal medullary, posterior chamber ophthalmic surgeries will need DAPT discontinued • If P2Y12 inhibitor stopped, try to maintain aspirin • Restart the P2Y12 inhibitor post surgery (within 24 hours if possible, with 300mg bolus).
Strategies for Peri-op Management of DESPost Op issues • Resumption of DAPT as soon as possible • Using bolus dose of P2Y12 inhibitor • Intensive post–op monitoring if off DAPT • Prompt evaluation and intervention for stent thrombosis or any bleeding
Strategies for Peri-op Management of DESPost-op Stent Thrombosis • Usually presents as ST elevation MI • Fibrinolytic therapy is contraindicated • Primary PCI is the treatment of choice • When DAPT is interrupted prematurely for surgery it should be done at hospitals with 24 hour cath/PCI availability
Strategies for Peri-op Management of DESPost-op Bleeding • Platelet transfusion is only somewhat effective with P2Y12 agents • It’s not effective with Integrlin or Aggrastat, but with short ½ life normal platelet function is restored in about 6 hours • RBC transfusion as needed
Summary/Highlights • Timing of elective surgery • What to do with medications • Stopping anti-platelet meds (DAPT) • When to restart • Post operative concerns
Timing of Surgery Post-Stenting • Bare Metal Stents • Wait 30-45 days for elective surgery • But do it prior to 6 months (or wait > 1 yr) • Drug Eluting Stents • Wait at least 6 months for elective surgery • Ideal - 1 year for elective surgery (??)
Anti-platelet medications • If possible continue all anti-platelet medications • If Plavix (P2Y12) must be stopped do so 5-7 days before surgery and re-start ASAP with 300-600mg bolus • REALLY try to continue aspirin, if stopped do so 5 days before and restart ASAP
Anti-platelet medications • Consider “bridging therapy” with IV administration of IIb/IIIa inhibitor (short half-life) in certain situations