Download
1 / 26
260 likes | 281 Views
Explore the NCEP ATP III cholesterol guidelines and updates with insights on risk factors, cardiovascular risk assessments, and statin therapy for high-risk patients. Learn about the 5 major clinical trials impacting cholesterol management and treatment options.

E N D
NCEP ATP III Cholesterol Guidelines and Updates • Anoop Agrawal, M.D. • Med-Peds Continuity Clinic • Baylor College of Medicine
Background • Adult Treatment Panel of the National Cholesterol Education Program issued their third guideline for cholesterol management in 2001 - known as ATP III. • Since publication, 5 major clinical trials of statin therapy have been published. • This has resulted in an addendum to ATP III published in July 2004. • Next update (ATP IV) expected in 2009.
Background cont. - The 5 studies: • Heart Protection Study - revealed 25% reduction in mortality regardless of baseline LDL levels • ALLHAT - did not show statin benefit in those with HTN; result attributed to use of pravastatin as study drug • PROVE IT - intensive statin therapy following acute coronary syndrome is superior • PROSPER - demonstrated statin benefit even in the elderly • ASCOT-LLA - LDL lowering with atorvastatin had considerable CVD risk reduction in those with multiple CVD risk factors. (in contrast to ALLHAT)
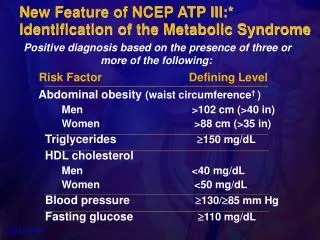
NCEP Major Risk Factors • Classification of an individual’s risk for cardiac events is based upon five risk factors: • smoking • hypertension • low HDL (<40) • family history- 1st degree relative with MI <55yo for male, <65 yo for female • age: male >45 yo, female >55 yo • **HDL > 60: reduction of 1 risk factor
CVD Risk Assessment • Based upon the 10 year cardiovascular risk score. • >20% and/or coronary heart disease (CHD) equivalents: high risk • very high risk: CHD + other risk factors • 10-20% and 2+ risk factors: moderate high • <10% and 2+ risk factors: moderate risk • 0-1 risk factor: lower risk calculated using Framingham risk score
CHD Equivalents • What are the recognized Coronary Heart Disease equivalents? • Diabetes Mellitus • Peripheral Arterial Disease • Symptomatic Carotid Artery Disease (TIA or stroke of carotid origin) • Abdominal Aortic Aneurysm • 10 yr risk for CHD >20% with 2+ risk factors
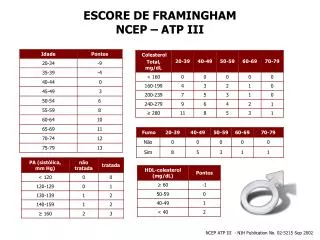
Example of Framingham risk assessment calculator • Found at www.nhlbi.nih.gov/guidelines/cholesterol • can also google ’10 year cvd’ and will be first hit
ATP III Guidelines - 2004 *for moderate high risk patients with 100-129 baseline or after TLC: initiation of LDL lowering drug to achieve LDL <100 mg/dl is an option Adapted from Third report of the National Cholesterol Education Program (NCEP) Expert Panel on detection, evaluation, and treatment of high blood cholesterol in adults (Adult Treatment Panel III). Circulation 2002; 106:3143; with modifications from Grundy, SM, Cleeman, JI, Merz, CN, et al, Circulation 2004; 110:227.
Case V.H. • What is your recommendation for managing his cholesterol?A. TLC and simvastatin 20mgB. TLC and vytorin 10/40C. TLC and atorvastatin 40mgD. TLC for 3 months, then reevaluate • V.H. is a 60 year old male with CAD, DM II, and tobacco use. His baseline lipid panel is: TLC: therapeutic lifestyle changes
Case V.H. cont... • Mr. V.H.’s 10 yr CVD risk places him at >20%. Having CAD and 2 additional risk factors promotes him to the very high risk group. • His LDL goal is <100 with the option to achieve LDL < 70 mg/dl • In selecting a statin for high risk patients, intensity of therapy needs to achieve at least 40% reduction in LDL. • Remember not all statins are created equal.
2004 Addendum to ATP III • For High Risk: • Prior to addendum: The treatment goal for high-risk patients was an LDL < 100. Drug therapy was initiated only if LDL ≥ 130. • UPDATE: Overall goal is still an LDL < 100. There is a therapeutic option to set the goal at an LDL < 70 for very high-risk patients • Also initiate drug therapy if LDL ≥100; also have the option to add on if baseline already < 100.
Which of the following do you recommend?A. TLC only, she is at goalB. simvastatin 20mgC. omega-3 fatty acidsD. ezetimibe 10mg Case M.H. • M.H. is a 48 yo female with uncontrolled HTN (today 160/80) and a smoker. Her FH is significant for her mother with heart disease at age 61. She currently is not on lipid therapy. Her baseline lipid panel
Case M.H. continued... • What is her classification and goal LDL? • Based on her 10 yr risk score (11%) she is Moderate High risk, goal LDL < 130. But <100 is therapeutic option if baseline is already <130 and has uncontrolled risk factors. • Simvastatin 20mg would be sufficient to reach goal. • Why not ezetimibe (Zetia)? • Not first-line choice. Recent study (ENHANCE) showed zetia did lower LDL, but did not show slowing or regression of atherosclerosis.
2004 Addendum to ATP III • In Moderate High Risk: • Prior to addendum:The treatment goal was an LDL < 130, and drug treatment was recommended if LDL is 130 or higher. • UPDATE:The overall goal for moderately high-risk patients is still an LDL < 130. There is a therapeutic option to set the treatment goal at an LDL < 100, and to use drug treatment if LDL is 100-129.
2004 Addendum to ATP III • For both High and Moderate High: • Prior to addendum: Guidelines did not explicitly emphasize achieving a certain percentage lowering of LDL cholesterol. • Update: Advises that the intensity of LDL-lowering drug treatment in high-risk and moderately high-risk patients be sufficient to achieve at least a 30-40% reduction in LDL levels.
Each doubling of the dose of a statin, gives only an additional 6% reduction of LDL from initial baseline at which statin was initiated. Comparison of the efficacy of statin drugs
Case 3: Myalgias due to statin • A 56 yo female is complaining about myalgias due to her therapy with simvastatin 40mg. Her LDL is 146. Her goal LDL is <100. Which of the following are viable options? • a. reduce simvastatin to 20mg nightly • b. change to atorvastatin 40mg nightly • c. change to niacin • d. change to ezetimibe 10mg daily
Case 3 : Myalgias due to statin • a: Myalgias are dose dependent response to statins. Lowering the dose may prevent the symptoms. In this case, reducing the dose would not help reach goal • b: Myalgias are not seen with every statin; no clear reason for this patient-variable response. If patient agreeable, then try another statin. Atorvastatin 40mg will be more effective than simvastatin 40mg at reaching goal. • c: Niacin does not help lower LDL. • d: Ezetimibe is a option if patient refuses to try another statin or has myalgias with another statin
Case 3: Myalgias due to Statin • Clinical Pearls: • Frequency of statin-related myalgias with normal CK is approximately 10-20%. • Occurrence of myalgias is dose-related • Ezetimibe can lower LDL by 20% • Bile acid-resins are another alternative treatment option (colesevelam)
New FDA: Simvastatin • Data fro SEARCH trial • incidence of adverse CV events was 25.7% in simvastatin 20mg group vs. 24.5% in 80 mg group • Myopathy - 52 patients in 80-mg group vs. 1 in the 20mg group • Rhabdo - 44
FDA: Simvastatin labeling • Simvastatin is more prone to drug interactions than other statins because it is extensively metabolism by CYP3A4 • Rates of rhabdomyolysis with simvastatin 80mg is higher than with 80mg atorvastatin or 20/40mg of rosuvastatin.
Summary • Recent updates affect patients in high and moderate high risk categories. • Encourages more aggressive lipid control due to evidence of significant reduction in vascular events regardless of baseline level of LDL. • Some LDL goals are still optional. In general, patients with high and moderate high risk are targeted to lower LDLs.
Summary • When initiating statin therapy, initial dose should target at least a 30-40% reduction in LDL. • If goal LDL requires more than a 50% reduction of baseline, then goal will likely be unattainable with current options.