Download
1 / 41
470 likes | 1.07k Views
Level II Training Clinical Documentation Improvement. DoIM – Hospitalists 7/09/14 Presented by: Catherine P orto, MPA, RHIA, CHP Exec. Director HIM, UNMH ICD-10 Executive Project Lead & Erlinda Smith, CCS CDI Provider Education & Kayode Balogun CDI Program Development - Precyse.

E N D
Level II TrainingClinical Documentation Improvement DoIM – Hospitalists 7/09/14 Presented by: Catherine Porto, MPA, RHIA, CHP Exec. Director HIM, UNMH ICD-10 Executive Project Lead & Erlinda Smith, CCS CDI Provider Education & KayodeBalogun CDI Program Development - Precyse
UNMMG Coding Staff – Current State UNMMG Professional Fee Coding: • Assign ICD-9-CM diagnosis code (for that visit) • Assign CPT procedure Codes (for that visit) • Evaluation & Management (E/M)codes for provider services • Procedure codes –for provider fees
UNMMG Provider Coding • 4 Day Hospital Stay (Evaluation &Management) • Day 1 = Initial Hospital Care (CPT 99223) • Charge = $514.00 • wRVUs = 3.86 • Day 2 = Subsequent Hospital Care/Follow up (CPT 99233) • Charge = $265.00 • wRVUs = 2.00 • Day 3 = Subsequent Hospital Care/Follow up (CPT 99233) • Charge = $265.00 • wRVUs = 2.00 • Day 4 = Hospital Discharge (CPT 99239) • Charge = $269.00 • wRVUs = 1.90 • Total Provider Charges = $1,313 • Total Provider wRVUs = 9.86
UNMH Coding Staff • Hospital (Facility) Coders are responsible for Facility Coding for the hospitals and clinics: • Assignment of one DRG Code derived from: • One Principle Diagnosis (ICD-9-CM) • All Secondary Diagnoses (ICD-9 & capturing all present on admission (POA) diagnoses) • One Principle Procedure (ICD-9-PC) • All Secondary Procedures (ICD-9-PC) • Any & all Co-morbidities & Complications(CC & MCCs) • Assignment of the DRG
Assignment of the MS-DRG • DRG(Diagnosis Related Grouping) • One DRG is assigned for each Inpatient stay • Using all diagnoses and procedures codes • Includes codes for all complications & comorbidities (CCs and MCCs) • DRGs are assigned a relative weight (RW) • RW is the calculation of resource consumption • Used to determine payment
MS-DRG Financial Impact • Relative weight (RW): Number assigned to each account based on the DRG assigned. The higher the RW, the sicker the patient. • 1: Average • <1: Below average • >1: Above average • Case Mix Index (CMI): The average of all relative weights for apatient population (Month, Year, etc.) for any given period of time.
Secondary Data UsesThe role of the APR-DRGs • APR-DRG (All-Payer Refined DRG-3M Software) • Calculates Severity of Illness (SOI) • Calculates Risk of Mortality (ROM) • Based on diagnoses, procedures and • Complications & Co-morbidities (CC and MCCs) • SOI & ROM scales (APR-DRG & UHC scale) • 1. Minor • 2. Moderate • 3. Major • 4. Extreme
POA and HAC There is a BIG difference in whether a condition was: • POA: Present on Admission – documentation in the H&P or progress notes after a definitive diagnosis is made—whether each condition was present on admission (provider’s best clinical judgment) • Does this patient have a pressure ulcer (where)? OR • HAC: Hospital Acquired Condition • For some selected conditions (diagnoses) that were not present on admission, but were acquired during hospitalization, the case may be paid as though the secondary diagnosis is not present • Fracture occurring during the IP stay • Diabetic Ketoacidosis (MCC) not present on admission • Foreign object retained after surgery • Vascular Catheter-Associated Infection • Surgical Site Infection
Documenting Questionable Diagnoses Provider should document all possible, probable, or suspected conditions – this communicates what the provider is thinking. • Example: • Professional fee Dx: Cannot code R/O-- rolls back to coding a symptom • IP - Possible Sepsis, r/o sepsis: Sepsis coded as though it exists • Sepsis ruled out: Sepsis would not be coded—IP remember to confirm prior to discharge or in the discharge summary • Pneumonia vs. CHF: Both can be coded (IP); pro fee-- codes to a symptom (i.e. chest pain, shortness of breath etc.)
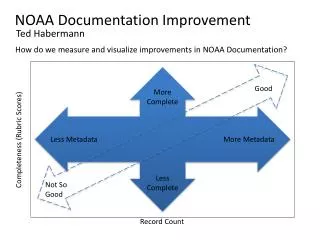
Mission: Meaningful Clinical Process “Telling the Patient’s Story” Clinical Information is used by clinicians for “telling the story” for this episode of care. Primary uses of clinical documentation: • The Documentation storycritical for patient care • The Medical Record is a communication tool among care providers • The Documentation should tell/demonstrate the clinical pathway to diagnoses Many times the story is lost in our current “cut and paste” or more forward world or documentation.
Secondary Uses of Clinical Information “As Documented in the EMR” Secondary Clinical Information/Data Uses: • Disease & Operative Indexing for research (ICD & CPT codes) • Validates the patient care provided • Serves as a legal document of the care provided • Drives Revenue/Reimbursement (Coding) • Permits accurate comparisons to other providers/institutions/national benchmarks • Identifies the quality and efficiency of the care we give. Computer extractions of: • Quality Indicators (PQRS) • Meaningful Use Data (MU) • Compliance/Regulatory Standards (TJC, CMS, DOH) • Metrics used for Value Based Purchasing
Why does CDI Matter?Medicine is Under The Microscope • Cost per patient • Resource utilization • Length of stay • Complication Rates • Morbidity Scores • Mortality Scores • Outcome Analysis • Payer Audits
Physician Profiling • Hospital Report cards • Healthgrades, Delta Group, Leapfrog • Medicare Physician Data (since 2007) • Federal and state regulatory agencies (e.g. OIG) • The Joint Commission (TJC) • Centers for Medicare and Medicaid Services (CMS) • Quality Improvement Organizations (QIO)
ICD-10: Advancing Healthcare… The Federal Government through CMS is driving the healthcare industry to upgrade diagnosis and procedure coding standards (ICD-10) by October 1, 2015. ICD-10 Changes Implications • Pervasive Impacts • Diagnosis codes and procedure codes flow through mission critical operational systems and analytical tools • Alignment of technology remediation with business and technology strategies • Business process reengineering, training and change management is essential • Comprehensive Benefits • Quality Measurement • Public Health Disease Surveillance • Clinical Research • Organizational Monitoring and Performance • Reimbursement • ICD-10 • (International Classification of Diseases version 10) • The ICD is the international standard diagnostic classification for general epidemiological, health management purposes and clinical use. • ICD-10 CM & PCS is an upgrade of the U.S. developed Clinical modification (ICD-9-CM) of Diagnosis and Procedure Codes, first adopted in 1979. Significant Increase in Clinical Granularity ICD-9 CM (Diagnosis) ICD-10 CM (Diagnosis) 3-5 characters alphanumeric 3-7 alphanumeric characters >14,000 unique codes > 68,000 unique codes ICD-9 CM (Procedure) ICD-9 CM (Procedure) ICD-10 CM (Procedure) 3-4 characters numeric 7 alphanumeric characters > 4,000 unique codes 5 digits > 72,000 unique codes > 4,000 unique codes
The ICD-10-CM diagnosis code set is a full replacement of the ICD-9 code set that will provide additional granularity for diagnosis and procedure codes. This additional granularity is the primary driver of value. The Basics of the ICD-10-CM Change An Example of Structural Change ICD-9 ICD-10-CM . . Etiology, anatomic site, manifestation Category Category Etiology, anatomic site, manifestation Extension X X X X X X X X X X X X . An Example of One ICD-9 code being Represented by Multiple ICD-10 Codes Type 1 diabetes mellitus with diabetic neuropathy, unspecified E 1 0 4 0 One ICD-9 code is represented by multiple ICD-10 codes . Type 1 diabetes mellitus with diabetic mononeuropathy E 1 0 4 1 . Type 1 diabetes mellitus with diabetic amyotrophy E 1 0 4 4 . Diabetes mellitus with neurological manifestations type I not stated as uncontrolled 2 5 0 6 1 . Type 1 diabetes mellitus with other diabetic neurological complication E 1 0 4 9 The industry expects that mapping ICD-9 and ICD-10 codes will be a complex task
The Basics of the ICD-10-PCS Change An Example of Structural Change ICD-9 ICD-10-PCS . Section Body System Root Operation Approach Device Qualifier Body Part X X X X X X X X X X X An Example of One ICD-9 code being Represented by Multiple ICD-10 Codes One ICD-9 code is represented by multiple ICD-10 codes . Total hip replacement 8 1 5 1 The ICD-10-PCS is an American procedure coding system that represents a significant step toward building a health information infrastructure that functions optimally in the electronic age.
ICD-10 Coding Snapshot: Diabetes Scenario • A 68 y/o male has type I diabetes with diabetic chronic kidney disease stage 3, is being seen for regulation of insulin dosage. The patient has an abscessed right molar, which was determined, in part, to be responsible for elevation of the patient’s blood sugar. • ICD-10 codes: • E10.22 Diabetes type 1 with CKD • N18.3 CKD Stage 3 • K04.7 Abscess Tooth • Z79.4 Long term drug therapy, insulin
ICD-10 Physician Education • Don’t need to turn doctors into coders • We Need good documentation habits • We Need specialty specific documentation education • We need to Begin the process of education now for ICD-9 and incorporate ICD-10 issues into the education as we prepare for Oct. 1, 2014 (Now 2015)
April Discharges – OrthoMajor Joint Replacement – Lower Extremity
Sepsis • SIRS Criteria • Assess for 2 or more • (Fever) Temp > 38⁰C or < 36⁰C • (Tachycardia) HR > 90 • (Tachypnea) Resp rate > 20 or pa CO₂ < 32 • (Leucocytosis/Leukopenia) WBC > 12K, < 4K, or > 10% bands
SIRS: Suspected Infection If infection is known: • Document organism and site • Document whether infection is present on admission • May document possible, probable, likely or suspected sepsis • Complete Sepsis M-Page • Determine Sepsis Severity
Sepsis Severity Sepsis • Lactate levels documented • No organ dysfunction • No hypotension Severe Sepsis • Lactate levels • Organ failure • Organ dysfunction must be linked to the Sepsis * (Occult) Septic Shock (Written as Septic Shock) • Lactate levels • No hypotension Septic Shock Written as Septic Shock • Hypotension • Refractory to IV fluids *see organ reference pages
SMITE Bundle Basic SMITE Bundle • Lactate q 4h x2 • Blood Culture 3. Antibiotics within 1 h 4. Fluids 5. Re-evaluate as needed Advanced SMITE Bundle Basic Bundle Plus: • Fluids bolus • CVP • Vasopressors
Severe Sepsis : Organ Dysfunction Documentation of • (Encephalopathy) Altered mental status • (Acute kidney injury)Creat levels/abnormal labs • (Acute liver failure) Abnormal LFTs/Total Bili • (Coagulopathy) INR level documented • (Acute respiratory failure) Hypoxemia and/or hypercapnia *Please refer to organ reference for detailed documentation suggestions
Case Study #1 MS DRG –178 Respiratory Infections & Inflammations w CC PDX:Cystic Fibrosis with pulmonary manifestations SDX: protein-calorie malnutrition. GERD, several other dx SOI level: 3 ROM level: 2 DRG Wt. 1.4403 DRG Reimb: $13,091.09 Additional documentation in chart CDI Queries for: nutrition note documentation, malnutrition related to CF. Pt with BMI 15.9 on high calorie diet and clinimixi at 80 cc an hr for nutritional support. Malnutrition documented on PN. CDI query for the severity of the malnutrition. If provider agreed with query and documents severe protein calorie malnutrition. MD DRG-177 Respiratory Infections & Inflamationsw MCC SOI level: 3 ROM level: 3 DRG WT. 2.0549 DRG Reimb: $18,677.24
Case Study # 2 MS DRG –872 Septicemia or Severe Sepsis w/o MCC PDX:Septicemia due to E coli SDX: protein calorie malnutrition, DM without complications type II, acute pancreatitis SOI level: 3 ROM level: 2 DRG Wt. 1.0687 DRG Reimb $8,120.74 Additional documentation in chart: Sepsis with AMS CDI Queries for: Specific type of Encephalopathy . If provider agrees and documents metabolic encephalopathy MS DRG-871 Septicemia or Severe Sepsis W MCC SOI level: 3 ROM level: 3 DRG WT.1.8527 DRG Reimb: $14,078.15
Department Training Schedule • Level I Training – Completed by April 30, 2014 • Level II Training – Completed by June 1, 2014 • Level III Training – Expectation: You are here • Dept Champion (s) Complete 1:1 training by June 1, 2014 • All Dept. Specialty Training to be completed in June/July 2014 for ICD-10: Date to be determined by UNM HSC (RFP Vender selection underway 6/1/14 • Metrics & Measures part of Monthly Department Meetings by June 2014 • Top Dx/Tip Sheets & All Staff Trained by Dept/Div Champions by June 30, 2014
Upcoming in Fall 2014: • Dept./Div. Specialty-Specific CDI Training • Vendor Proposals for Level III Training chosen by RFP Committee. Next steps: • Top vendors on-site to demonstrate their sub-specialty training method & tools – week of July 21 • Encourage All Dept/Division Champions and anyone else interested to attend • Dept/Division – Specialty Specific ICD-10 Documentation Sessions to be scheduled in the Fall of 2014 (following UNM HSC approval of vendor and purchase)
Contacts UNMH Coding & Clinical Documentation ErlindaSmith, CCS UNMH Coding Educator (Inpatient) EVSmith@salud.unm.edu KayodeBalogun, MD, CCS CDI Program Manager, UNMH kbalogun@salud.unm.edu Catherine Porto, RHIA, MPA, CHP Exec. Director HIM cporto@salud.unm.edu CDI Information to be posted on the following web site: https://hospitals.health.unm.edu/intranet/HIM Provider Documentation and ICD-10 Tab