Download
1 / 17
170 likes | 176 Views
This study examines the differences in Medicare patient selection and outcomes between hospital-based and freestanding nursing homes, and explores potential factors influencing these differences. The study utilizes regression analysis, propensity score approach, and modified propensity approach to control for selection bias and other covariates. The findings reveal substantial differences in outcomes, suggesting potential variations in care and institutional factors. However, there may be other unobserved factors that contribute to these differences.

E N D
Controlling for Medicare Patient Selection into Hospital-based versus Freestanding Nursing Homes Sally Stearns, Kathleen Dalton, Mark Holmes Cecil G. Sheps Center for Health Services Research, UNC-Chapel Hill Susanne Seagrave Centers for Medicare & Medicaid Services AcademyHealth Annual Research Meeting, June28 2005 Funding source: Medicare Payment Advisory Commission
Industry Background • Skilled nursing facilities (SNFs) • About 14,000 certified for Medicare in 2000 • 85% freestanding (FS) • 75% are for-profit • 15% hospital-based (HB) • 17% are for-profit • Hospital-based facilities are different: • Medicare length of stay half as long • Cost per day 50% to 100% higher • Better staffing ratios • Patients thought to be different • 1998: Cost-based -> Prospective Payment
Research Issues • Study question: • For clinically similar patients, do HB and FS settings differ in: • Medicare covered length of stay • rate of hospital readmission • rate of discharge to home within 30 days? • Research Challenge: • Controlling for selection • Standard regression models often unsatisfactory in removing bias from unmeasured case mix differences
Possible Analytic Approaches • Use regression analysis of outcome variable with many explanatory measures tominimize selection bias • Propensity score approach (PS) • Construct a prediction model for HB = f (X) • Group observations according to predicted p(HB) • Model outcome within group • Analogous to adding more measures (i.e., lots of interactions) • Instrumental variables (IV) • Being addressed elsewhere
Data Source • Nursing home stay-level data set • Claim from initial qualifying hospitalization • Claim from Medicare-covered nursing home stay • Detailed patient status data from 5, 14, 30, 60- and 90-day MDS nursing home assessments • Claim from any re-hospitalization • Date of death (followed through 2002) • We added facility & market-level variables • Very large data set (648,306 stay observations from 7/2000 – 6/2001 after exclusions)
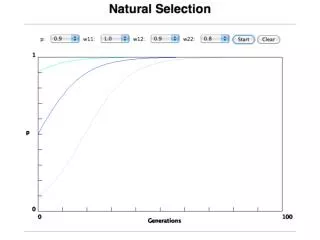
Driving Force for Referral Decision • Single strongest predictor of HB referral is coming from a hospital that operates its own SNF. • Referral decision appears to be very different when coming from a hospital that does not have operate its own SNF
The probability of HB referral is different in a hospital with a SNF versus one without. It appears to be a different choice process.
Outcome Regression Model • Where HB is a dummy and X is: • Patient characteristics • Sociodemographics • Clinical info from hospital stay and MDS data • Variables capturing prognosis • SNF characteristics • Market area characteristics
Stratified Propensity Model • Referral Equation: • Use only observations from hospitals with SNFs • Outcome Equation • For J=1,…,5 groups of observations based on predicted probability of being referred to a hospital-based SNF
Modified Propensity Approach • Usual propensity score approach problematic • Balancing achieved with respect to p(HB) but not with respect to all covariates. • Continued need to control for covariates in outcome models. • Simplified approach: divide p(HB) into 5 strata • Groups may not be as clinically similar as would be desirable • But should provide a rough approximation of formal propensity groups to demonstrate impact
HB Referral Equation Results • Used only patients from hospitals with SNFS • Outcome estimations used full sample • Good candidates for fast recovery and discharge home are preferentially selected into HB SNFs • Most important factors related to prognosis, rather than specific diagnoses, procedures or RUG groups
Summary of Results/Issues • Substantial differences in unadjusted outcomes greatly reduced by controlling for observed variables. • Propensity stratification approach provided modest reduction in some groups • Useful to identify heterogeneity in treatment effects • Limitations • Potential endogeneity of “short stay” assessment • Other unobserved variables
Conclusions • Selection of certain types of patients into HB versus FS facilities occurs • Differences in outcome remain: • May be attributable to care or institutional differences in treatment • May be explained by other unobserved factors