Download
1 / 158
1.59k likes | 1.97k Views
Chapter 11 Blood vessels. Vascular wall responses Congenital Anomalies Atherosclerosis Arteriosclerosis Hypertension Aneurysms. Vasculitides Raynaud “phenomenon” Veins Lymphatics Tumors Interventions. TOPICS. NORMAL VESSELS Arterial walls are thicker than veins

E N D
Chapter 11 • Blood vessels
Vascular wall responses Congenital Anomalies Atherosclerosis Arteriosclerosis Hypertension Aneurysms Vasculitides Raynaud “phenomenon” Veins Lymphatics Tumors Interventions TOPICS
NORMAL VESSELS • Arterial walls are thicker than veins • To accommodate pulsatile flow and higher blood pressures.
Structure of blood vessels • Tunica intima • Endothelium and connective tissue • Tunica media • Smooth muscle and elastic tissue • Tunica externa or tunica adventitia • Connective and elastic tissue
Arteries • Large arteries are elastic (conducting) arteries – pressure reservoirs • Medium arteries are muscular (distributing) arteries – more smooth muscle • Contraction or relaxation of muscle changes the size of the lumen, and so controls the blood pressure in the vessel.
Capillaries • Only a single layer of endothelium and a basement membrane • Connect arterioles and venules • Functional part of system • True capillaries begin at a precapillary sphincter which controls blood flow through the capillary
Veins • Relatively thin; less elastic • Larger in diameter than arteries • Have valves to prevent backflow of blood • Flow to heart is assisted by contraction of skeletal muscles
Veins have larger diameters, larger lumina, and thinner, less well-organized walls • veins are more prone to dilation, compression, and easy penetration by tumors and inflammatory processes.
Lymphatics are thin-walled, endothelium-lined channels that drain excess interstitial tissue fluid eventually returning it to blood via the thoracic duct. Lymphatic flow also contains mononuclear inflammatory cells and a host of proteins; by passing through lymph nodes,
Functions of the lymphatics • 1. lymphatics constitute an important pathway for continuous sampling of peripheral tissues for infection. • 2.These channels can also disseminate disease by transporting microbes or tumor cells from distant sites to lymph nodes and eventually to the systemic circulation
The main cellular components of the walls of vessels are: 1) endothelial cells 2) smooth muscle cells 3) pericytes (the cells normallyarranged along capillaries and venules)
Endothelial cells: • a)serve as a semipermeable membrane, • b) regulate thrombosis, thrombolysis and platelet adherence, • c) influate vascular tone and blood flow, • d) metabolize hormones, • e) regulate immune and inflammatory reactions, • f) modify lipoptoteins in the artery wall, • g)regulate the growth of other cell types, including smooth muscle cells.
Endothelial injury is critical to the formation of thrombi, to the initiation of atherosclerosis and the vascular effects of hypertension and other disorders !!
Endothelial dysfunction • Endothelial activation
Pathology of blood and lymphatic vessels The term endothelial dysfunction is often used to describe several types of potentially reversible changes in the functional state of endothelial cells that occur in response to environmental stimuli.
The term endothelial activation reflects alterations in gene expression and protein synthesis. Inducers of endothelial activation include cytokines and bacterial products (which cause inflammatory injury and septic shock), hemodynamic stress and lipid products (involved in pathogenesis of atherosclerosis), advanced glycosylation of end products (involved in pathogenesis of diabetes), as well as viruses, complement components and hypoxia..
Activated endothelial cells also elaborate adhesion molecules, other cytokines and chemokines, growth factors, molecules of the major histocompatibility complex (MHC), procoagulant or anticoagulant factors and vasoactive molecules that are involved either in vasoconstriction or in vasodilatation
2)Smooth muscle cells are capable: a)to mediate vasoconstriction, By Nitric oxide b) to mediate vasodilatation, c) to synthesize the collagen, elastin, and proteoglycans, d) to elaborate the growth factors and cytokines, e) to proliferate, and f) to migrate to the intima. 3) Pericytes have role as supportive and connective elements.
Diseases of arterias • A) Congenital anomalies • B) Atherosclerosis • C) Hypertensive vascular disease • D) Inflammatory disease – Arteritides (Vasculitides) • E) Raynaud disease • F) Aneurysms a dissections
Congenital anomolies • AVM Arterio Venous malformations • Abnormal communication between the high pressure arteries and low pressure veins. • Usually congenital but acquried by trauma or inflammation. • Most often described in Brain as AVM • Asymptomatic or hemorrhage or pressure effect.
Diseases of arterias B. Atherosclerosis It is a generic term for three patters of vascular disease that have in common thickening and loss of elasticity of arterial walls: 1)Atherosclerosis– characterized by the formation of intimal fibrous plaques that often have a central core rich in lipid (fibrofatty plaques). 2) Mönckeberg medial calcific sclerosis – characterized by calcific deposits in medium-sized muscular arteries in persons older than 50 years. These medial lesions forming irregular medial plates or discrete transverse rings have much less clinical importance. 3) Arteriosclerosis – the hyaline and hyperplastic thickening of small arteries and arterioles which causes luminal narrowing and down stream ischemic injury.
Monckeberg arteriosclerosis (medial calcific sclerosis) involves the media of medium sized muscular arteries, most typically the radial and ulnar arteries, • persons older than 50 years of age. It does not obstruct arterial flow because the intima is not involved. • a. Ring-like calcifications in the media of the arteries are characteristic. • b. Stiff, calcific "pipestem" arteries result. • c. This form of arteriosclerosis may coexist with atherosclerosis, but it is distinct from and unrelated to it.
ARTERIO-SCLEROSIS • GENERIC term for ANYTHING which HARDENS arteries • Atherosclerosis (99%) • Mönckeberg medial calcific sclerosis (1%) • Arteriolosclerosis, involving small arteries and arterioles, generally regarded as NOT strictly being part of atherosclerosis, but more related to hypertension and/or diabetes
Hyaline Arteriolosclerosis. This vascular lesion consists of a homogeneous pink hyaline thickening of the walls of arterioles with loss of underlying structural detail and with narrowing of the lumen. • Present in • Elderly patients, whether normotensive or hypertensive, • patients with hypertension. • It is also common as part of the characteristic microangiography in diabetes .
HISTOPATHOLOGY ofESSENTIAL HYPERTENSION “HYALINE” = BENIGN HTN. “HYPERPLASTIC” = MALIGNANT HTN. SYS>200 1) ONION SKIN 2) “FIBRINOID” NECR.
Hyperplastic Arteriolosclerosis. Seen in • Malignant hypertension (typically, diastolic pressures over 120 mm Hg associated with acute cerebral and/or renal injury). • Hyperplastic arteriolosclerosis is associated with "onion-skin," concentric, laminated thickening of the walls of arterioles with luminal narrowing The laminations consist of SMCs and thickened, duplicated basement membrane.
In malignant hypertension, these hyperplastic changes are accompanied by fibrinoid deposits and vessel wall necrosis (necrotizing arteriolitis), particularly prominent in the kidney.
HYPERTENSION • “ESSENTIAL” 95% • “SECONDARY” 5%
Primary hypertension • Also called essential or idiopathic hypertension • 92- 95 % of all cases • No specific cause identified • Can happen with retention of sodium and water → increased blood volume. • Also low dietary potassium, calcium and magnesium intakes
Suspected causes • Interaction of genetics and environment • Overactivity of sympathetic nervous system • Overactivity of renin / angiotensin/ aldosterone system • Salt and water retention by kidneys • And others
SECONDARY • Renal • Acute glomerulonephritis • Chronic renal disease • Polycystic disease • Renal artery stenosis • Renal artery fibromuscular dysplasia • Renal vasculitis • Renin-producing tumors • Endocrine • Adrenocortical hyperfunction • (Cushing syndrome, primary aldosteronism, congenital adrenal hyperplasia, licorice ingestion) • Exogenous hormones (glucocorticoids, estrogen [including pregnancy-induced and oral contraceptives], sympathomimetics and tyramine-containing foods, monoamine oxidase inhibitors) • Pheochromocytoma, Acromegaly, Hypothyroidism (myxedema), Hyperthyroidism • Pregnancy-induced • Cardiovascular: Coarctation of aorta, Polyarteritis nodosa (or other vasculitis) • Increased intravascular volume • MISC: Increased cardiac output, Rigidity of the aorta, Neurologic, Psychogenic, Increased intracranial pressure, Sleep apnea, Acute stress, including, surgery
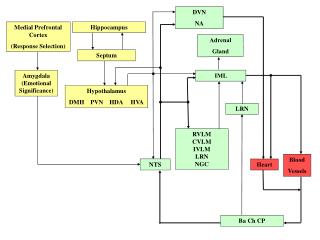
ReninAngiotensinAldosteroneAXIS (RAAS) • If the perfusion of the juxtaglomerular apparatus in the kidneys decreases, then the juxtaglomerular cells release the enzymerenin. • Renin cleaves an inactive peptide called angiotensinogen, converting it into angiotensin I. • Angiotensin I is then converted to angiotensin II by angiotensin-converting enzyme (ACE), which is found mainly in lungcapillaries. • Angiotensin II is the major bioactive product of the renin-angiotensin system. Angiotensin II acts as an endocrine, autocrine/ paracrine, and intracrine hormone.
GENETIC ACQUIRED
GENETICvs.ENVIRONMENTAL • GENETIC UN-CONTROLLABLE • ENVIRONMENTAL CONTROLLABLE • STRESS • OBESITY • SMOKING • PHYSICAL ACTIVITY • NaCl INTAKE
ATHEROSCLEROSIS(classical) • Etiology/Risk Factors • Pathogenesis • Morphology • Clinical Expression
FATTY STREAK (non-palpable, but a visible YELLOW streak) • 2) ATHEROMA (plaque) (palpable) • 3) THROMBUS (non-functional, symptomatic)
MAJORfactors • Hyperlipidemia • Hypertension • Cigarette Smoking • Diabetes Milletus
PATHOGENESIS • “atherosclerosis is a chronic inflammatory response of the arterial wall initiated by injury to the endothelium”
PATHOGENESIS • Chronic endothelial injury • LDL, Cholesterol in arterial WALL • OXIDATION of lipoproteins • Monocytes migrate endothelium* • Platelet adhesion and activation • Migration of SMOOTH MUSCLE from media to intima to activate macrophages (foam cells) • Proliferation of SMOOTH MUSCLE and ECM • Accumulation of lipids in cells and ECM
The mechanism of Hyperlipidemia contributing to Atherosclerosis • Endothelial impairment by chronic hyperlipidemia by increasing o2 free radicles production • Decay in NO • Impair vaso dilation • Impair endothelial functiuonOxidise the LDL
Fatty streak is the earliest lesion in Atherosclerosis • Composition • Atherosclerotic plaques • Components • Smoothmuscle cells macrophages and t cells • ECM • Intracellualr and extracellular lipids.
MORPHOLOGIC CONCEPTS • Macrophages (really monocytes) infiltrate • Intimal Thickening • Lipid Accumulation • Streak • Atheroma • Smooth Muscle Hyperplasia and Migration • Fibrosis • Calcification • Aneurysm • Thrombosis