Download

1 / 16
170 likes | 384 Views
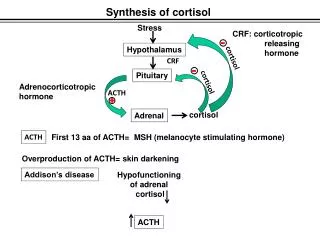
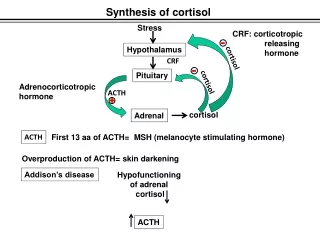
Cortisol and Aldosteron. Two hypothalamic peptides are the principal regulators of pituitary ACTH release , corticotropin releasing hormone (CRH) and arginine vasopressin. They act independently and synergistically.

E N D
Two hypothalamic peptides are the principal regulators of pituitary ACTH release , corticotropin releasing hormone (CRH) and arginine vasopressin. They act independently and synergistically. • CRH is a 41 A.A peptide secreted by the paraventicular nucleus which acts via the cAMP second messenger system . • AVP is a 9 A.A peptide synthesized by both the supraoptic and paraventicular nuclei , which acts by altering intracellular calcium ion channels . • Negative feedback by cortisol reduces the action of both CRH and AVP .
ACTH • ACTH is part of the 241 A.A precursor molecule proopiomelanocortin (POMC) . • POMC is unusual as a hormone precursor in that it is cleaved to release several hormonally active peptides including the endorphins and melanocyte stimulating hormones . POMC is normally only produced by the pituitary gland but it may also be produced in large quantities by certain malignancies giving rise to ectopic ACTH syndrome.
ACTH itself is comprised of 39 A.A with the biological activity residing in the N-terminal 24 moieties . ACTH . It transported unbound in plasma. It has a half-life of about 10 minutes and is unstable in plasma . ACTH stimulates the synthesis and release of glucocorticoid hormones by interacting with cell surface receptors on the adrenal cortex that stimulate the production of intracellular cAMP . Acute increases in the adrenal synthesis of cortisol occur with 3 minutes , principally by stimulating the activity of cholesterol esterase.
Chronic effects of ACTH include induction of transcription of the genes that encode steroidogenic enzymes and other factors • Fast feedback alters the release of hypothalamic CRH and CRH-mediated secretion of ACTH . Slow feedback results from reduced synthesis of CRH and AVP plus suppression of POMC gene transcription , which results in reduced ACTH synthesis .
Biosynthesis of cortisol • Cortisol is the major glucocorticoid synthesized in man in the inner two zones of the adrenal cortex under the direct controle of pituitary ACTH. • Cholesterol is the precursors for all steroid hormones synthesis. Cleavage of the cholesterol side chain liberates the so-called C-21 corticosteriods, further side chain cleavage yields the C-19 androgens and aromatization of the A ring result in the C-18 estrogens.
The biosynthesis of cortisol depends on stimulation by pituitary ACTH hormone which binds to its plasma membrane receptor and cause hydrolysis of cholesterol esters stored in lipid droplets and activation the enzyme desmolase (cytochrome P450 monoxygenase system) which is the rate limiting enzyme. • Approximately 95% of cortisol in plasma is bound to protein, mainly CBG. As cortisol concentration rises, the percentage of free cortisol also rise, indicating that CBG binding is saturable. Cortisol has a half-life in plasma of about 100 minutes. Cortisol is metabolized in the liver and other organs by a combination of reduction.
Cortisol has a major influence on gluconeogenesis by enhancing virtually every step in the gluconeogenesis pathway. At the same time, cortisol inhibits glucose uptake and metabolism in peripheral tissues. • Excess cortisol has a wide range of effects on the immune system causing overall suppression and providing a useful from of therapy. It is likely that at least some of these action are important in the control of the immune response in normal physiology.
Cortisol also influences the heart, vasculature, blood pressure, water excretion and electrolyte balance. Clinical disorders of cortisol secretion:-Hyposecretion of cortisol may occur as a result of: 1- adrenal gland destruction was often due to tuberculosis, auto immune disease is now the main cause of primary adrenal failure. Both cortisol and aldosterone production may be affected.
2- Secondary due to long-standing suppression and subsequent impairment of the hypothalamic-pituitary axis. • In the primary adrenal insufficiency, patients become hyponatraemic, due to lack of aldosterone which leads to pathological sodium loss by the kidney which results in a contraction of the extracellular fluid volume, causing hypotension and pre-renal uremia. • The hypovolaemia and hypotention stimulate AVP secretion, thus causing water retention.
In the secondary deficiencies of CRH and ACTH are often accompanied by deficiencies of other hypothalamic or pituitary hormones. • Hypersecretion of cortisol results in Cushing's syndrome.
ALDOSTERONE Renin is released from juxtaglomerular cells in response to decreased renal perfusion pressure . It is protease that uses angiotensinogen as its substrate . Angiotensinogen, a glycoprotein of more than 400 a. a , is synthesized in the liver . The renin liberates Angiotensin 1 from angiotensinogen . Angiotensin 1 is a short, 10 a.a peptide. It is the substrate for Angiotensin-converting enzyme (ACE) .
ACE is responsible for the removal of two amino acids from Angiotensin ǀ to produce the most potent known vasoconstrictor molecule , Angiotensin ǀǀ . In the kidney , Angiotensin ǀǀ affects blood flow, glomerular function , and by stimulation of aldosterone secretion which in turn affects sodium, potassium and hydrogen ion transport. These actions of Angiotensin ǀǀ are mediated through two different receptors: the AT1 receptor is G-protein-linked, whereas the AT2 receptor can inhibit protein tyrosine phosphatase activity .
Aldosterone is produced in the adrenal cortex, and is the major mineralocorticosteroid hormone in man . Its production is stimulated by increases in the plasma concentration of potassium . Aldosterone regulates electrolyte balance in the kidney , salivary glands , sweat glands and gastrointestinal tract . In the kidney , it increases the activity of the Na/K-ATPase that causes renal sodium retention and, in parallel, an increased excretion of potassium .