Download
1 / 32
320 likes | 573 Views
Late Preterm Birth as a Risk Factor for Neonatal Morbidity among Singleton Newborns Discharged Early. Kay M. Tomashek, MD, MPH Maternal and Infant Health Branch Division of Reproductive Health Centers for Disease Control and Prevention. Co-authors. Division of Reproductive Health, CDC

E N D
Late Preterm Birth as a Risk Factor for Neonatal Morbidity among Singleton Newborns Discharged Early Kay M. Tomashek, MD, MPH Maternal and Infant Health Branch Division of Reproductive Health Centers for Disease Control and Prevention
Co-authors Division of Reproductive Health, CDC Carrie Shapiro-Mendoza, PhD, MPH Massachusetts Department of Public Health Angela Nannini, FNP, PhD Wanda Barfield, MD, MPH Boston University School of Public Health Judy Weiss, PhD Milton Kotelchuck, MPH, PhD Gene Declerq, PhD Stephen Evans, MPH
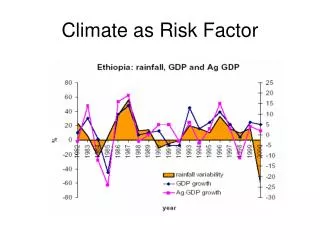
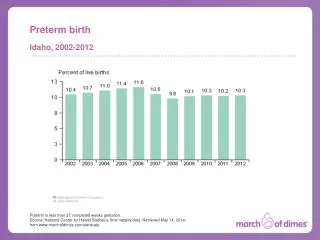
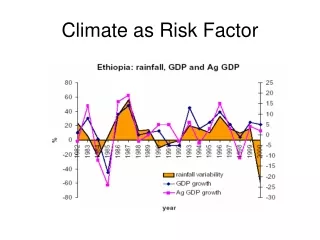
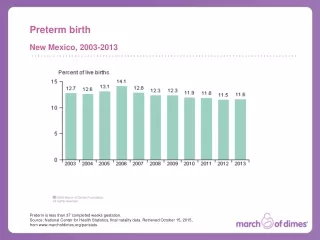
Background • Late preterm births (34–36 weeks gestation) are increasing • 8.5% of all US births in 2002 • Late preterm births account for 71% of all preterm births • Late preterm infants are at increased risk for mortality compared to term infants
Background • Late preterm newborns often receive routine care and are presumed low risk • Late preterm infants are premature infants • Little is known about neonatal outcomes among late preterm infants
Background • Early discharge (<48 hr stay after vaginal delivery) is a controversial topic • Studies divided as to associated risk • AAP recommends early discharge be limited to term infants • Understanding how late preterm infants are affected by discharge policies is essential for shaping policy and preventing morbidity
Study Objectives • Compare risk of neonatal morbidity between singleton late preterm and term newborns who were discharged early after vaginal delivery • Compare differences in principal diagnosis upon hospital readmission and timing of readmission between two groups
Study Design • Population-based cohort study using data from the Massachusetts Pregnancy to Early Life Longitudinal Database (PELL) • Longitudinally linked vital statistics (birth and death certificates), hospital discharge records, and observational stay records
Study Design • Definitions • Late preterm – 34 to 36 weeks gestation • Term – 37 to 41 weeks gestation • Early discharge – <2 night hospital stay
Study Population • Singletons between 34 and 41 weeks gestation who were vaginally delivered at a MA hospital between 1998–2002 and discharged early to home • Excluded • unmatched records • non-MA resident births • gestation unknown or implausible
Methods Data • 1998-2002 linked birth/death certificates, delivery hospital discharge records, neonatal hospital inpatient and observational stay records Outcomes • Hospital readmissions • Observational stays
Methods Analysis • Description of characteristics of late preterm and term infants • Comparison of risk of neonatal morbidity between late preterm and term infants • Calculated crude and adjusted risk ratios and 95% CI using modified Poisson regression • Stratified analysis by breastfeeding status
Results • Of the 15,089 singleton late preterm and 242,934 term infants who were vaginally delivered at a Massachusetts hospital to a state resident and discharged home • 6.7% late preterm and 10.0% term infants were discharged early
Results Proportion of infants with neonatal morbidity
Results Risk of Neonatal Morbidity Among Newborns Discharged Early After Vaginal Delivery *All models adjusted for gender and parity. All morbidity and observational stay models also adjusted for prenatal care utilization.
Percent Neonatal Morbidity by Breast Feeding Status and Gestational Age aRR 1.8 (1.2, 2.6) aRR 1.0 (0.6, 1.8)
Percent Re-admitted by Breast Feeding Status and Gestational Age aRR 2.2 (1.5, 3.2) aRR 1.1 (0.6, 2.2)
Neonatal Re-admission Diagnoses Among Infants Discharged Early Late preterm infants Term infants
Timing of readmission • Jaundice • 80% of all readmissions in 1st week for late preterm infants versus 56% for term infants • Day 3 of life most common day for admission • Infection • 10% of all readmissions in 1st week for late preterm versus 7% for term infants; 60% and 53% in the 2nd week • On average, late preterm infants presented nearly one week earlier than term infants
Limitations • Unable to link all records • Unable to account for all neonatal morbidity • Misclassification of gestational age • Validity of available indicators • Unable to measure residual confounding (e.g., home visits)
Conclusions • Among singleton infants discharged early, late preterm are at greater risk of neonatal morbidity than term infants • Being late preterm was associated with a nearly two-fold risk of neonatal hospital readmission • Our data suggest that risk may be present only for breastfed infants
Conclusions • Readmission rates for term infants were similar to those reported in the literature • There are no published studies of late preterm discharged early • However, study by Escobar found late preterm infants never admitted to NICU were 3 times more likely than term infants to be readmitted within 2 weeks of discharge
Conclusions • Jaundice and infection most common diagnoses upon readmission • Timing similar for jaundice • Late preterm infants with infection presented nearly one week earlier than term infants • This study illustrates the need for closer follow-up of late preterm infants discharged early • Further analyses are needed to understand the optimum timing for discharge after birth for healthy-appearing late preterm infants
Contact Info Kay M Tomashek, MD, MPH E-mail: kct9@cdc.gov Phone: 770-488-6272 Maternal and Infant Branch Division of Reproductive Health National Center for Chronic Disease Prevention and Health Promotion Centers for Disease Control and Prevention
Neonatal Re-admission Diagnoses Among late preterm Infants Discharged Early
Neonatal Re-admission Diagnoses Among Term Infants Discharged Early
Results • Jaundice was the principal diagnosis for 80% of all readmissions during the first week of life among late preterm infants, compared with 56% among term infants • Fifty percent of late preterm and term infants who were readmitted with a principal diagnosis of jaundice were readmitted by 4 and 3 days of age, respectively, and 75% were readmitted by 5.5 and 4 days of age. The most common day to be readmitted for jaundice among both late preterm and term infants was the third day of life.
Results • Infection accounted for 10% of readmissions in the first week of life and 60% in the second week among late preterm infants. • For term infants, these figures were 7% and 53%, respectively. • Among late preterm infants who were readmitted with a principal diagnosis of infection, 50% were readmitted by 11 days of age and 75% by day 15. • Among term infants readmitted with infection, 50% were readmitted by day 17 and 75% by day 23.