Download
1 / 72
781 likes | 1.34k Views
DIGESTIVE SYSTEM. By Dr SaminaAnjum. FORMATION OF PRIMITIVE GUT. Cephalocaudal folding Lateral folding. FORMATION OF PRIMITIVE GUT. Incorporation of endoderm lined cavity in embryo Yolk sac and allantois remain outside the body of embryo. DIVISIONS OF PRIMITIVE GUT.

E N D
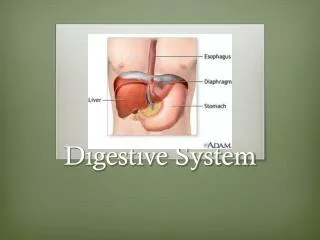
DIGESTIVE SYSTEM By Dr SaminaAnjum
FORMATION OF PRIMITIVE GUT • Cephalocaudal folding • Lateral folding
FORMATION OF PRIMITIVE GUT • Incorporation of endoderm lined cavity in embryo • Yolk sac and allantois remain outside the body of embryo
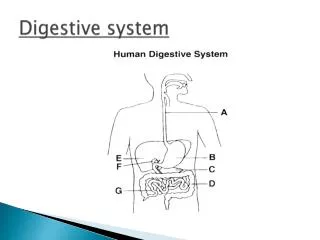
DIVISIONS OF PRIMITIVE GUT Foregut & hind gut are the blind ending tubes
Endoderm forms: • The epithelial lining of gut • Parenchyma of glands Visceral mesoderm forms: • Stroma of glands • Musculature of organs • Peritoneum
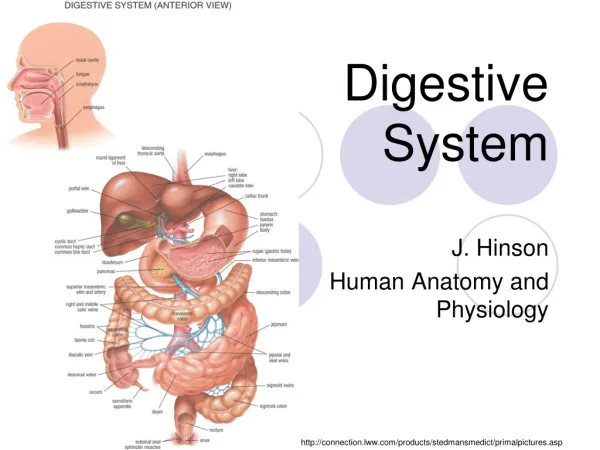
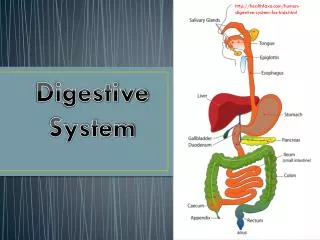
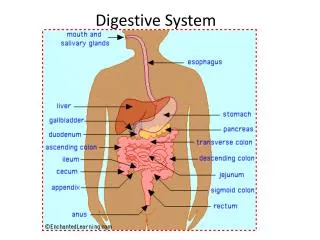
FOREGUT • The derivates of foregut are: • The primordial pharynx and its derivates namely, oral cavity, pharynx, tongue, tonsils, salivary glands and upper respiratory system. • The lower respiratory system. • The esophagus and stomach. • The duodenum, proximal to the opening of the bile duct. • The liver, biliary apparatus (hepatic ducts, gall bladder, bile duct and pancreas) • All these foregut derivatives, except the pharynx respiratory tract and most of the esophagus are supplied by celiac trunk.
Initially short, but with the descent of the heart and lungs, it lengthens rapidly. • The muscular coat & Innervation
Abnormalities Of Esophagus Tracheoesophageal fistula and atresia Polyhydramnios. Esophageal stenosis in the lower third. Congenital hiatal hernia occurs when the esophagus fails to lengthen sufficiently and the stomach is pulled up into the esophageal hiatus through the diaphragm.
Development of Stomach • Fusiform dilation of the foregut in the fourth week • Dorsal & Ventral mesenteries • The stomach rotates around a longitudinal and an anteroposterior axis.
The stomach rotates 90 degrees clockwise around its longitudinal axis, causing its left side to face anteriorly and its right side to face posteriorly.
Vagus nerves • During this rotation, the original posterior wall of the stomach grows faster than the anterior portion, this differential growth forms the greater and lesser curvatures.
The cephalic and caudal ends of the stomach originally lie in the mid line, but during further growth, the stomach rotates around an anteroposterior axis so that the pyloric part moves to the right and upward and cardiac portion moves to the left and slightly downwards.
Rotation about the longitudinal axis pulls the dorsal mesogastrium to the left and creates a space behind the stomach called the lesser sac. • This rotation pulls the ventral mesogastrium to the right.
The spleen primordium appears as a mesodermal proliferation between the two leaves of the dorsal mesogastrium during 5th week. • The posterior leaf of the dorsal mesogastrium and the peritoneum along this line of fusion degenerate. • Lienorenal and gastrolienal ligaments.
Initially pancreas grow in the dorsal mesoduodenum, but eventually its tail extends into the dorsal mesogastrium and is covered by peritoneum on its anterior surface only and therefore lies in a retroperitoneal position. • Secondarily retroperitoneal organs: pancreas
GREATER OMENTUM Forms by the dorsal mesogastrium as it bulges down and forms a double layered sac extending over transverse colon and small intestinal loops. Later it layers fuse and forms a single sheet hanging from the greater curvature of stomach. The posterior layer of greater omentum fuses with the mesentery of transverse colon.
FALCIFORM LIGAMENT & LESSER OMENTUM Forms from the ventral mesogastrium. Its derivatives are: • Falciform ligament- free margin contains left umbilical vein; obliterates after birth to form ligamentum Teres hepatis • Lesser omentum- Right free margin(hepatoduodenal ligament) contains portal triad and forms the roof of the epiploic foramen
Abnormalities Of Stomach • Pyloric stenosis is one of the most common abnormalities of the stomach in infants which is believed to develop during fetal life. • Occurs when circular muscle hypertrophies. • Extreme narrowing of the pyloric lumen and the passage of food is obstructed, resulting in severe projectile vomiting.
DEVELOPMENT OF DUODENUM • The terminal part of the foregut and the cephalic part of the midgut form the duodenum. • The junction of the two parts is directly distal to the origin of the liver bud.
Due to the rotation of the stomach, the duodenum takes on the form of a C-shaped loop and rotates to the right. • Ultimately, the duodenum swings from its initial midline position to the right side of the abdominal cavity
Once developed, the hepatic and cystic ducts connect to the duodenum by the common bile duct . • The entrance of the bile duct into the small intestine gradually shifts from an initial anterior positionto a posterior one and passes behind the duodenum.
The duodenum and head of the pancreas press against the dorsal body wall and the right surface of the dorsal mesoduodenum fuses with the adjacent peritoneum and subsequently disappear.
The dorsal mesoduodenum disappears entirely except in the region of the pylorus of the stomach where a small portion of the duodenum (duodenal cap) retains its mesentery and remains intraperitoneal
During the 2nd month, the lumen of the duodenum is obliterated. However, the lumen is recanalized shortly thereafter. Celiac Artery Superior mesenteric Artery Cont…
///LIVER & GALL BLADDER • Hepatic diverticulum appears - middle of 3rd week as an outgrowth of the endodermal epithelium at the distal end of foregut • Liver bud consists of rapidly proliferating liver cells that penetrate the Septum Transversum
Cont… • With further proliferation connection between liver bud & foregut narrows to form bile duct • A small ventral outgrowth is formed by bile duct , this outgrowth give rise to gallbladder and the cystic duct.
Hepatic sinusoids • Formed by vitelline & umbilical veins • Epithelial Liver cords • Differentiate into parenchyma & form lining of biliary ducts • Mesoderm of septum transversum • Hematopoietic cells • Kupffer cells • Connective Tissue cells
Mesoderm of septum transversum becomes membranous forming lesser omentum & falciform ligament • Mesoderm on the surface of the liver differentiates into visceral peritoneum except on its cranial surface. • Here, the liver remains in contact with the rest of the original septum transversum which form the central tendon of the diaphragm - Bare area of liver
6th week Hematopoiesis • 10th week • Weight of the liver - 10% of total body weight • 12th week • Bile formed by hepatic cells • Bile duct formed & bile can enter the GIT • Last two months • Hematopoietic function reduced • Weight of the liver only 5% of total body weight
Development of Pancreas In dorsal mesentery
When duodenum rotates to right and becomes C- shaped, the ventral pancreatic bud moves dorsally and comes to lie immediately below and behind the dorsal bud. • Later, the parenchyma and the duct systems of the dorsal and ventral pancreatic buds fuse.
DERIVATIVES OF PANCREATIC BUDS & DUCTS • The ventral bud • the uncinate process • inferior part of the head of the pancreas. • The dorsal bud • The remaining part of the gland. • The main pancreatic duct of Wirsung, together with the bile duct enters the duodenum at the site of the major papilla. • The distal part of the dorsal pancreatic duct • The entire ventral pancreatic duct. • Accessory pancreatic ductof Santorini • The proximal part of the dorsal pancreatic duct. The entrance of the accessory duct is at the site of the minor papilla.
Third month • pancreatic islets (of Langerhans) develop from parenchymal cells. • Fifth month • Insulin secretion • Glucagon and somatostatin-secreting cells also develop from parenchymal cells. • Splanchnic mesoderm surrounding the pancreatic buds forms the pancreatic connective tissue.
MIDGUT • Begins distal to the entrance of bile duct into duodenum and terminates at the junction ofright two-thirds of the transverse colon with the distal third. • Superior mesenteric artery
In the 5th week midgut • Is suspended from the dorsal abdominal wall by a short mesentery. • Communicates with the yolk sac through vitelline duct until the tenth week
Development of midgut: Is characterized by rapid elongation of gut and its mesentery to form the primitive intestinal loop. • Midgut loop has • Cephalic limb--- Distil part of duodenum, jejunum and part of ileum • Caudal limb--- Lower portion of ileum, cecum , appendix, ascending colon and proximal 2/3rd of transverse colon
Physiological umblical Herniation Cause: Due to rapid growth and expansion of liver, abdominal cavity becomes smaller • Movement of intestinal loops into EEC in the umbilical cord during 6th week.
ROTOATION OF MID GUT • The midgut loop during herniation in the umbilical cord, rotates 90 ° counterclockwise (when viewed from the anterior aspect) around the axis of the superior mesenteric artery. • The cranial limb swings down and right while the caudal limb swings up and left • During rotation, the cranial limb of the midgut elongates and forms jejunal-ileal loops while the expanding cecum sprouts as vermiform appendix .
Cont… • Additional rotation at 180° counterclockwise when intestinal loops return into abdomen during 10th week. • Total rotation of midgut= 270° counterclockwise
RETRACTION OF HERNIATED LOOPS Causes: • Regresssion of mesonephric kidney • Reduced growth of liver • Expansion of abdominal cavity During 10th week herniated intestinal loops return to the abdominal cavity. Proximal portion of jejunum is the first part to reenter the abdominal cavity. Later remaining loops settle more and more to right.
The caecal diverticulum is the last part of the gut to reenter the abdominal cavity, temporarily lying in the right upper quadrant directly below the right lobe of the liver. • The caecal bud descends to the right iliac fossa, placing the ascending colon and the hepatic flexure on the right side of the abdominal cavity. As the appendix forms during the caecum's descent, it frequently lies posterior to the caecum (retrocaecal) or posterior to the colon (retrocolic).
The derivatives of the midgut • The small intestine, including most of the duodenum • The cecum, appendix, ascending colon and the right two-thirds of the transverse colon
FATE OF MESENTERIES • The mesentery of the primary intestinal loop becomes very twisted with the movements of the bowel. Dorsal mesentery of small intestine twist around the origin of superior mesenteric artery when caudal limb of loop moves to right side of abdomen • Mesenteries of ascending and descending colon press against the peritoneum of the posterior abdominal wall, fuse & degenerate so that these organs become secondarily retroperitoneal.
Cont… • The mesentery of transverse mesocolonfuses with the posterior wall of the greater omentum. • The appendix, lower end of the cecum and sigmoid colonretain their free mesenteries.