Download
1 / 53
530 likes | 740 Views
Neurology. Study of disorders of the nervous system. What is the nervous system?. Central Nervous system (CNS) Brain Spinal Cord Peripheral Nervous system Nerves to and from body parts to the CNS. Autonomic Nervous System. Breathing Digestion Heart rate Blood Pressure Sweating etc.

E N D
Neurology Study of disorders of the nervous system
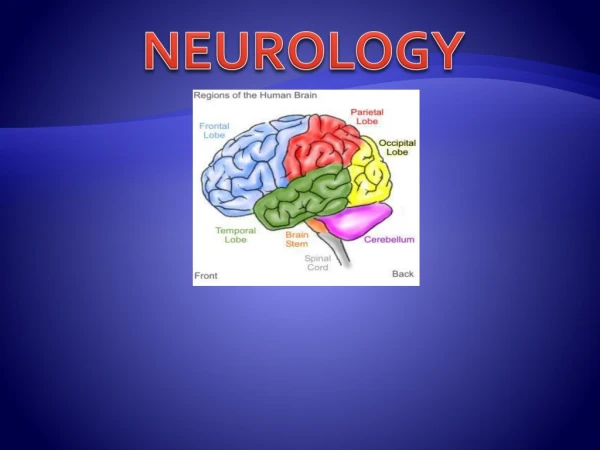
What is the nervous system? • Central Nervous system (CNS) • Brain • Spinal Cord • Peripheral Nervous system • Nerves to and from body parts to the • CNS
Autonomic Nervous System • Breathing • Digestion • Heart rate • Blood Pressure • Sweating etc.
Disciplines frequently interacting with Neurology • NeuroSURGERY • Physical Medicine & Rehabilitation (PM&R) • Psychiatry • Family Practice • Medicine • Pediatrics
Common Reasons Why Referrals are made to Neurology • Diagnosis and treatment • Headaches • Weakness or paralysis • Seizures • Mental Delay or deterioration • Memory Loss • Change in Personality
What Happens in the Neurology Clinic of Consult? • History • Neurological Exam • Confirmatory Tests
History • THE MOST IMPORTANT PART !! • Why are you here? • NO GOOD - my doctor sent me, or for a neurological check !! • The questions asked during the history ar based upon the concern for being there!
Neurological Exam • Consists of several parts, HOWEVER IS ALSO FOCUSED BY THE PRESENTING CONCERN !! • Mental Status (Language, memory, affect) • Cranial Nerves • Motor (strength, muscle mass, tone) • Deep Tendon Reflexes (DTR’s – WHY??) • Sensory (Perception of touch, pain) • Coordination & Balance (walking, manual dexterity)
Confirmatory Tests • CT Brain or Spinal Cord Scan • MRI Brain or Spinal Cord Scan • Angiography • Electroencephalogram (EEG) • Electromyogram (EMG) • Ultrasound • Blood and Genetic Tests
Computerized Tomography (CT SCAN) • Relatively inexpensive • Quick • Very good for acute bleeding • Good for fractures & bones • BUT significant X-Ray exposure
Magnetic Resonance Imaging (MRI) • Can be more informative • No x-ray exposure BUT • Much more expensive • Takes longer, may need sedation • Can induce claustrophobia
Electroencephalogram (EEG) • In some ways similar to an EKG (ECG) of the heart • Records the tiny electrical currents emitted by the brain • About thirty wires are pasted to the scalp for about 30-60 minutes • Harmless • Especially valuable in seizure disorders and epilepsy
Electromyogram (EMG) • Electrical recording of the peripheral nerves and muscles • Invaluable for neuropathiesand muscle disease • Needle exam, also delivery of small electric shock to see they travel • Harmless, BUT not too comfortable
Delayed (Slow) Intellectual and / or Motor Development • Why not sitting, Walking? • No or Abnormal talking • Is it both or just one or these • Commonly a combination or the two
Intellectual impairment (mental retardation) • A result of ANYTHING which harms the brain • Genetic • Brain malformations • Lack of oxygen • Infection • Trauma • Environment, lack of stimulation • Toxin (ALCOHOL, drug, Pb, Hg)
Management of Intellectual Impairment • Early referral to therapy • Correct cause where possible • Genetic counseling
Abnormal Motor Development • When profoundly weak, muscle disease, muscular dystrophy • Stiff, poor coordination, Cerebral Palsy
Cerebral palsy (CP) • Cerebral = head or brain • Palsy = abnormal muscle function, weakness, coordination, tremor
Cerebral Palsy • A RESULT OF ANYTHING which harms the brain • Genetic • Brain malformations • Lack of oxygen • Infection • Trauma (Birth or post natal) • Environment, lack of stimulation
Cerebral Palsy What Does it Look Like? • Abnormal motor development - delay • Weakness • Stiff (or limp) • Abnormal posture & movement
Spasticity and Dystonia = stiffness • Often the predominant feature of CP • Can contribute to orthopedic deformity • Interferes with function & care • Can be painful
Management of Spasticity • Drugs - valium, baclofen, dantrium • Indwelling pump for intrathecalbaclofen • Surgery - selective dorsal rhizotomy (SDR)
Additional Management of CP • Feeding issues • Surgery to correct secondary orthopedic deformities, especially painful hip dislocation • Adaptive equipment, standers, wheelchairs, powered wheelchairs • Communication devices
Abnormally Large Head • Can be the result of: • Blood clot (extradural hematoma) • Thick skull • Hydrocephalus **
What is Hydrocephalus? • Excessive fluid (CSF) INSIDE of the brain. • Caused by: • Birth deformity (Meningomyelocoel) • Genetic • Infection or bleed • Drugs (seizure meds)
Management of Hydrocephalus • Observation • Medication - Diamox • Surgery - Ventriculo-peritoneal (VP) shunting
Problems with CP Shunts • Infection (about 3%) • Obstruction (resulting in headaches, vomiting, enlarging head, death) • Outgrowing the length of the peritoneal catheter
Duchenne Muscular Dystrophy • X-linked recessive, decr dystrophin • 1 / 3-8,000 males, onset 3-6 yrs • WEAKNESS, difficulty climbing stairs • Abnl tests: CPK, EMG, dystrophin • Stop walking abut 12 years • May live to 3rd decade
EpilepsyCharacterized primarily by having seizures • More than one, unprovoked seizure • Seizure – transient, usually sudden disruption of cerebral function • i.e., shaking, paralysis, abnormal speech, staring
Epilepsy • A RESULT OF ANYTHING which harms the brain • Genetic • Brain malformations • Lack of oxygen • Infection • Trauma (Birth or post natal) • Environment, lack of stimulation • Brain tumor **
Seizures • Usually confirmed by EEG • Often completely controlled with medication (AEDs) about 50% • Another 25% much improved with drugs (one or more) • Some benefitted by seizure surgery and / or vagal nerve stimulator
Management of Seizures • Requires follow-up, seizure diary, AE of meds, drug levels. Usually several times per year, usually for years. • Focused history at each clinic visit • Special issues if pregnant
Headaches • Occur in both Children & Adults • Great Majority are NOT due to tumors! • Most are Migraine, Tension, or Cluster • When the histories are typical and the examination is normal, Ct or MRI brain scans usually are not necessary. • At least 10% of children & adults have HA • Frequently there is a positive family history
Management of Headaches • Prophylaxis: • diet, biofeedback,propranolol,Depakene, antidepresant, topiramate, • Acute Attack: • ergotamine, triptan (5-HT agonist-sumatriptan)
Brain Tumors • Occur both in children & adults, however the types vary by age • Although most headaches are NOT due to tumors, many brain tumors present with headaches. • Other symptoms: vomiting, failure to thrive & weight loss, visual impairment, ataxia, neurologic deficits, seizures,
Brain Tumors • Tumor types differ by age (more primaries in kids, metastatic in adults) • Symptoms similar- headache, visual changes, seizures, neurol deficits
Work-up of Brain Tumors • Neurological and Eye exam • Imaging – MRI or CT scans, angiography
Management of Brain Tumors • Stabilize and decrease intracranial pressure with steroids, shunting • Surgical excision or tumor reduction • Radiation and/or chemotherapy • Immunologic reduction (gliomas, melanoma)
Stroke • More common in adults, but also in kids • Syndrome with rapid onset of symptoms & signs(seconds or minutes) loss of CNS function • Transient Ischemic Attacks (reverse < 24 hours = “TIA”) & Reversible Ischemic Neurological deficits
Problems Which Could Look Like a Stroke • Diabetic Coma and hypoglycemia • Seizure • Head Injury • Complicated Migraine • Transient Global Amnesia
Causes of Stroke • Thrombosis & occlusion of vessels • Emboli – something traveling in vascular supply (usually clot) to occlude • Hemorrhage – berry aneurism, hypertension, abnl blood vessel (AVM) • (Risk factors SMOKING, obesity, diet, hypertension, family history)
Work-up of Stroke • CT / MRI brain scan • CT angiogram • MRI angiogram • Traditional angiogram